Playlist
Show Playlist
Hide Playlist
Osteopathic Treatment: Elbow Joint and Neurovasculature

-
Slides Osteopathic Considerations of the Upper Extremity.pdf
-
Reference List Osteopathic Manipulative Medicine.pdf
-
Download Lecture Overview
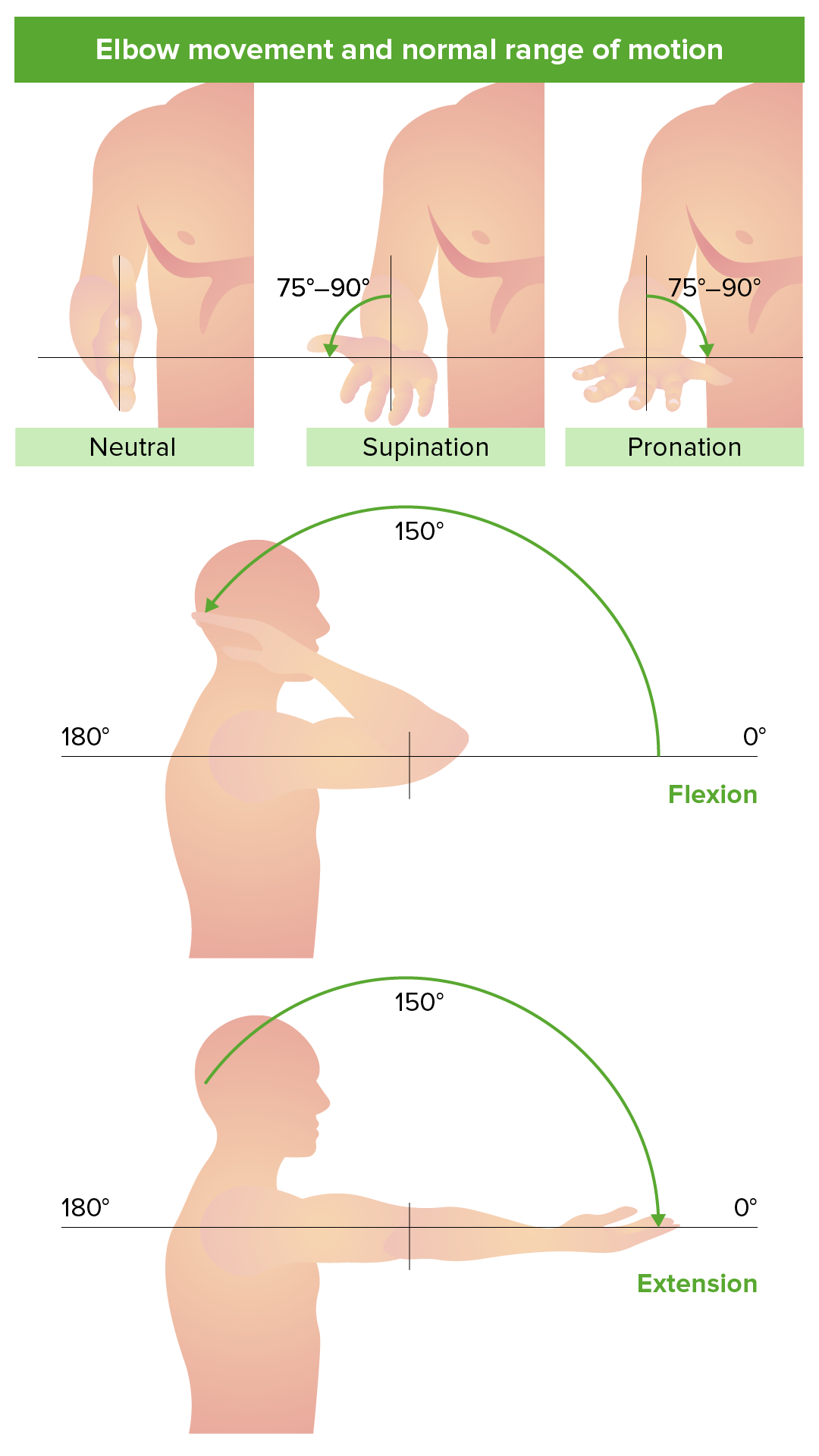
00:00 We're going to move on to the elbow now. 00:03 The elbow is another hinged joint . It is made up of the humerus. 00:08 You'll have the medial epicondyle and the lateral epicondyle. 00:12 We'll also talk about the bony attachments including the radius and the ulna that's making up the elbow joint. 00:19 The ligaments that hold the elbow together are typically strong ligaments. 00:24 You have the radial collateral ligament, the ulnar collateral ligament, the annular collateral ligament and the interosseous membrane holding the elbow together. 00:36 These four are generally tight. They're a little bit looser in infants and maybe an issue more in kids than in adults. 00:46 But when we look at the elbow, I want to talk about range of motion. 00:50 Extension is generally to 0 degrees, sometimes 5 degrees extra, flexion 130-145. Pronation goes to 75 degrees. 00:59 Supination goes to 85 degrees. That's the elbow motion. 01:03 When we talk about pathologies, I just wanted to mention four which is lateral epicondylitis, medial epicondylitis, the tennis elbow and golfer's elbow, radial head dysfunction, and collateral ligament injuries. 01:19 Starting with lateral epicondylitis, this is elbow pain on the outside that radiates down the forearm due to repetitive motion of sports. 01:30 You'll feel the pain in the wrist as well. 01:33 A provocative test is called Cozen's test. 01:36 It's when you have the elbow in full extension and you extend their wrist against their resistance. 01:45 If you have pain, that's a positive test. 01:48 We will do strain counterstrain for lateral epicondylitis, finding the tender point on the lateral aspect. 01:56 You can also do muscle energy, having the patient use resistance against the elbow in order to free up motion of the elbow. 02:05 Medial epicondylitis is a very similar problem on the inside. 02:09 It's generally elbow pain that radiates to the dorsum of the forearm due to repetitive finger and wrist flexion. 02:18 It can also happen from wrist pronation especially when the elbow is flexed. 02:24 So that's a tennis elbow. 02:26 Provocative tests are when you get pain during resistance and pain with wrist flexion with passive wrist extension. 02:35 Those are things you want to check to see if there is a tennis elbow. 02:39 It is an overuse injury. Treatment is first and foremost rest, stop doing what's causing the problem. Ice can help. 02:46 Analgesic can help. Steroids can help. 02:48 We do manipulative procedures as well, strain counterstrain, muscle energy, myofascial release, and facilitated positional release. 02:58 I want to talk about radial head dysfunction as well. 03:00 More common in kids than adults. 03:02 It is a radial head dislocation that happens from a fall with an outstretched arm who are being pulled up by somebody lifted by the arms with a weak ligament that allows the radial head to be pulled out. 03:15 They'll be nursing the arm and not using the arm. 03:19 On examination, you’ll want to assess the range of motion of the joint. Notably, they’ll be unable to supinate or pronate the arm. 03:28 It is easily treatable. It's more an awareness and a diagnosis being made. 03:33 Management is putting it back into place. It doesn't require surgery at first. 03:37 The osteopathic portion of treatment is loosening up the muscles prior to putting it back into place, and using muscle energy to get the posterior head back into place or the anterior radial head put back into place. 03:52 Either one can occur. 03:53 The next item to talk about is medial and lateral collateral ligament injuries. 03:59 These are when you have swelling or inflammation of the ligaments on the medial or lateral aspect of the elbow. 04:07 Provocative tests are looking at the valgus or varus stress as applied to it. 04:13 Knowing that when you push, what does the patient look like? Do they feel uncomfortable? You want to see if there's pain or increased laxity in that area, if it feels loose and out of socket. If you do, that's something that you want to rest as well and let the tendon have time to heal. We can do muscle energy techniques to treat the hypertonicity, to help relax the muscle and enhance motion, and give it time to heal but rest. Anti-inflammatory and bracing are also very important aspects of treatment. 04:44 In the elbow, we worry about the neurovascular bundle and the radial nerve getting entrapped or other areas in the elbow being interrupted. 04:57 For a radial nerve entrapment, we do worry when there is pain just distal to the lateral epicondyle with paresthesias, numbness and tingling in the hand due to the impingement. 05:11 This may be a medical emergency and needs to be addressed right away. 05:15 There are osteopathic approaches to treatment in the meantime. 05:19 But again, the definitive treatment needs to be arrived at. 05:22 Cubital tunnel syndrome is ulnar nerve entrapment on the medial side with numbness and tingling coming down towards the fifth digit with medial elbow tenderness. 05:35 This will have a positive Tinel's sign. 05:37 When you tap on it, are you going to elicit the numbness and tingling down the hand. 05:44 A positive test is when the symptoms are reproduced with the tapping. 05:50 Again, osteopathic intervention is the hypertonicity of the muscle, the stretching of the muscle and trying to loosen the muscles up so that the symptoms will go away and the patient will feel better. 06:01 The last neurovascular entrapment is median nerve entrapment which is the pronator syndrome, when you have an anterior interosseous syndrome with pain and tingling down the forearm. 06:14 Pronator syndrome affects the carpal tunnel-like symptoms. 06:19 It causes symptoms in the hands which are worse with pronation. 06:24 Again, myofascial release and counterstrain are the osteopathic interventions of choice.
About the Lecture
The lecture Osteopathic Treatment: Elbow Joint and Neurovasculature by Tyler Cymet, DO, FACOFP is from the course Osteopathic Treatment and Clinical Application by Region. It contains the following chapters:
- Elbow Joint
- Elbow Dysfunction
- Elbow Joint – Lateral Epicondylitis
- Elbow Joint – Medial Epicondylitis
- Elbow Joint – Radial Head Dysfunction
- Elbow Neurovasculature
Included Quiz Questions
Which of the following musculoskeletal problems at the elbow is assessed with the Cozen's test (or resisted wrist extension test)?
- Lateral epicondylitis
- Medial epicondylitis
- Anterior radial head dysfunction
- Proximal ulna dysfunction
- Posterior radial head dysfunction
Which of the following special provocative tests assesses the elbow for medial collateral ligament injury of the elbow?
- Valgus stress test
- Varus stress test
- Flexion stress test
- Extension stress test
- Yergason's test
A 32-year-old professional gamer presents to the clinic with numbness and tingling from the right elbow and radiating along the medial aspect of his right forearm to the little finger. Tapping the right wrist over the median or ulnar nerves does not reproduce the numbness and tingling; however, tapping the medial aspect of the right elbow just posterior to the medial epicondyle does reproduce the numbness and tingling. What is the likely diagnosis?
- Cubital tunnel syndrome
- Carpal tunnel syndrome
- Pronator syndrome
- Radial nerve entrapment
- Median nerve entrapment
Author of lecture Osteopathic Treatment: Elbow Joint and Neurovasculature

Tyler Cymet, DO, FACOFP
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
