Playlist
Show Playlist
Hide Playlist
Dix-Hallpike & Epley Maneuver Test

-
Slides 11 VertigoDizziness Neuropathology II.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
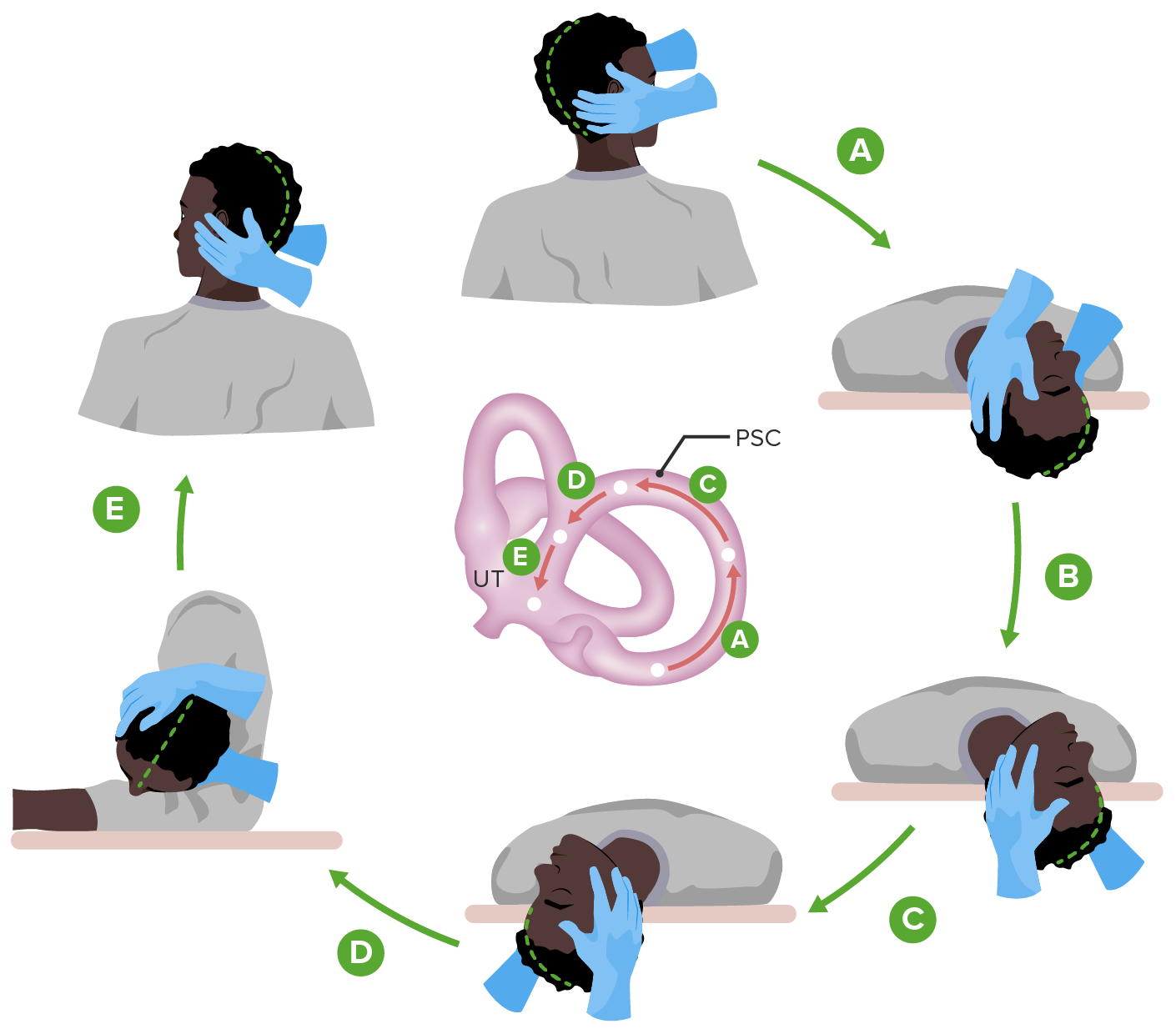
00:00 Here, we have vestibular neuronitis. 00:03 An acute unilateral peripheral vestibulopathy. 00:07 No evidence of inflammation. 00:09 Sudden or spontaneous vertigo associated with nausea and vomiting. 00:13 Symptoms will peak within 24 hours. 00:16 Resolves over days or weeks. 00:18 And unilateral nystagmus may be seen. 00:20 It can be suppressed by visual fixation. 00:24 That’s the clinical pearl here. 00:26 It can be suppressed by actual visual fixation. 00:29 This is known as your vestibular neuronitis. 00:32 What is labyrinthine concussion? It’s a head injury in which maybe perhaps there was or wasn’t a skull fracture. 00:41 Maybe associated with hearing loss and tinnitus. 00:45 Infarction: If there’s a problem with the vertebrobasilar system including your posterior inferior cerebellar artery, anterior inferior cerebellar artery, or maybe perhaps even your superior cerebellar artery. 00:58 Associated with brainstem signs including cranial nerve, and we have weakness, ataxia. 01:04 The central-type nystagmus: Pure vertical or pure horizontal, may be bilateral. 01:11 Are not suppressed by visual fixation. 01:14 That’s important for you to pay attention to here once again. 01:16 Not suppressed by visual fixation. 01:19 This is the central type of nystagmus. 01:22 What is Ménière's disease? Episodic vertigo with nausea and vomiting. 01:28 Fluctuating, but progressive hearing loss. 01:32 Tinnitus and sensation of fullness in the ear, your clinical pearl here is fullness in the ear and caused by increased endolymphatic volume or perhaps pressure. 01:43 Ménière's disease. 01:46 Perilymphatic fistula: As the name implies, a fistula. 01:51 Where? Abrupt onset of vertigo then persists episodically. 01:58 Often precedes by hearing a pop in the affected ear with sneezing, coughing, or blowing or straining. 02:06 A fistula, a perilymphatic, can be treated with rest or a fat patch if refractory. 02:13 Pop, perilymphatic, if that helps you. 02:18 BPPV, benign positional paroxysmal vertigo. 02:23 This is episodic vertigo, however, triggered by head movement. 02:27 Episodes are brief, but severe. 02:29 Associated with latency, finite duration and fatigue. 02:35 Often associated with severe nausea and vomiting caused by floating calcium carbonate crystals in the endolymph. 02:42 Pathology here, calcium carbonate actually floating in your endolymph. 02:47 Characteristic downbeating torsional nystagmus on Dix-Hallpike testing. 02:55 Downbeating torsional nystagmus. 03:00 It can be rapidly treated with what’s known as your Epley repositioning maneuver. 03:06 Here, what we have known as benign positional paroxysmal vertigo. 03:11 So what is the Dix-Hallpike or Epley maneuver? The Dix-Hallpike maneuver can be done while examining a patient who doesn't have vertigo symptoms at rest. 03:20 It tests for canalithiasis (or calcium crystals) of the posterior semicircular canal, which is the most common cause of BPPV (or positional vertigo). 03:29 It is performed by having the patient sit on the exam table, with their neck extended and turned 45 degrees to one side. 03:35 Instruct the patient to keep their eyes open, then help them to rapidly lie supine with their neck still extended so that the head hangs over the edge of the table. 03:42 Observe for signs of nystagumus or symptoms of vertigo for 30 seconds. 03:46 Then have the sit up quickly again, observe for another 30 seconds for nystagmus. 03:51 If the test is not already positive, then repeat with the head turned into the opposite direction. 03:55 The eply mameuver can be taught to patients who are experiencing vertigo at home. They lie on their backs and tirn their head side to side as shown in this depiction. 04:01 They lie on their backs as shown in this picture, and turn their heads from side to side. 04:05 This helps to dislodge the crystals and move them out of the posterior canal. 04:08 What are pearls for vertigo? Tinnitus and hearing loss accompanied peripheral vertigo. 04:15 Diplopia, dysarthria, and other brainstem signs point to a central cause. 04:22 Isolated vertigo is almost never caused by brainstem ischemia. 04:27 And BPPV, benign paroxysmal positional vertigo, is the most common cause of new onset vertigo. 04:36 And I just walked you through the Epley maneuver.
About the Lecture
The lecture Dix-Hallpike & Epley Maneuver Test by Carlo Raj, MD is from the course Vertigo and Dizziness. It contains the following chapters:
- Vertigo
- Dix-Hallpike/Epley Maneuver & Vertigo Pearls
Included Quiz Questions
Which of the following is the cause of benign paroxysmal positional vertigo?
- Calcium carbonate crystals in the endolymph
- Oxalate crystals in the endolymph
- Calcium carbonate crystals in the external ear
- Oxalate crystals in the external ear
- Calcium carbonate crystals in the perilymph
Which of the following is the cause of Ménière disease?
- Increased endolymphatic volume
- Decreased endolymphatic volume
- Decreased perilymphatic volume
- Increased perilymphatic volume
- Fracture of stapes
Which of the following statements regarding vestibular neuronitis is the MOST accurate?
- Nystagmus can be suppressed by visual fixation.
- Tinnitus is a prominent symptom.
- It carries a grave prognosis.
- It is a chronic and recurrent disease.
- Symptoms resolve within minutes.
The Epley maneuver is used to treat which of the following conditions?
- Benign paroxysmal positional vertigo
- Ménière disease
- Vestibular neuronitis
- Perilymphatic fistula
- Labyrinthine concussion
Author of lecture Dix-Hallpike & Epley Maneuver Test

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
