Playlist
Show Playlist
Hide Playlist
Distal Predominant Muscular Dystrophies

-
Slides Distal Predominant Muscular Dystrophies.pdf
-
Download Lecture Overview
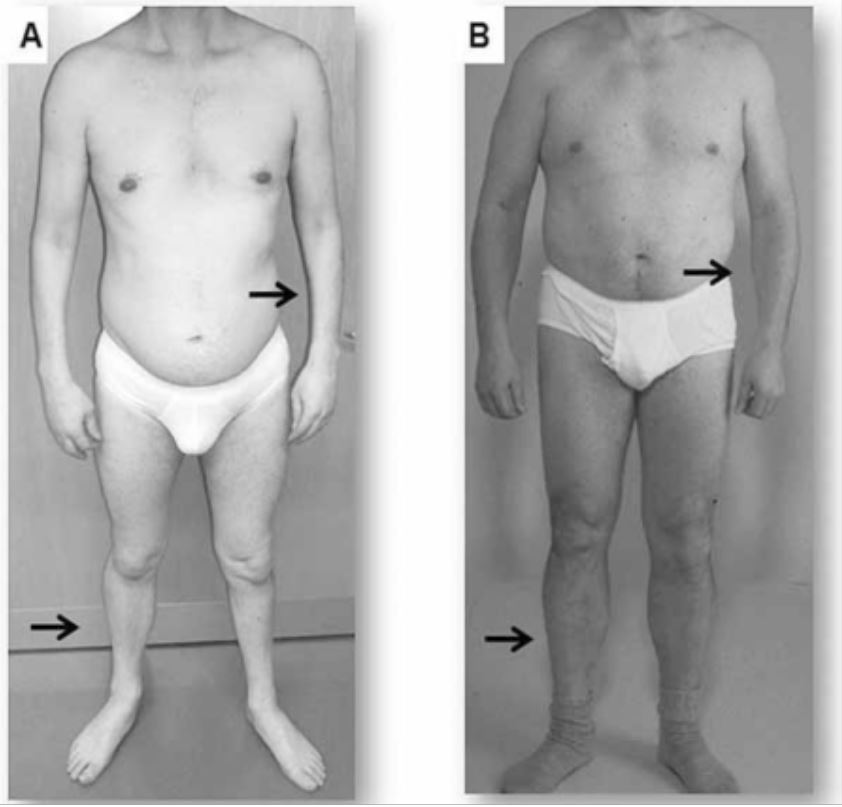
00:01 In this lecture, we're going to learn about the distal predominant muscular dystrophies and specifically talk a lot about myotonic dystrophies. 00:12 So what are the myotonic dystrophies and what is the distribution that we see in both myotonic dystrophies and distal predominant muscular dystrophies? Well, as the name implies, the symptoms are distal. 00:22 So we see weakness in the distal upper extremities, the hands, wrist extensors and wrist flexors, as well as the distal lower extremity, difficulty with foot drop and utilizing and maneuvering the foot. 00:37 In some of these conditions, and specifically the myotonic dystrophies which is the most important of the distal predominant muscular dystrophies. 00:44 We also see respiratory and cardiac muscle involvement and some symptoms in the face. 00:50 And that's an important piece to understand about these conditions because they can be recognized on physical exam. 00:57 So let's talk about the two myotonic dystrophies which are the prototypical distal predominant muscular dystrophies. 01:05 And we're going to learn about Myotonic Dystrophy 1 and Myotonic Dystrophy 2. 01:10 DM1 which is not to be confused with diabetes mellitus. 01:14 This is Myotonic Dystrophy Type I is an inherited muscular dystrophy. 01:19 And here the inheritance pattern is a trinucleotide repeat. 01:24 So it's not X-linked, it's not autosomal dominant, it's not autosomal recessive. 01:28 This is a trinucleotide repeat disorder and results from this CTG repeat. 01:35 Patients present with a number of muscle disorders, muscle weakness disorders that can include prominent facial weakness. 01:45 And this is important that facial weakness is one of the first things we see on exam and sometimes the thing that is accused us in on a clinical vignette. 01:54 Patients may have ptosis, or open mouth as a result of bifacial weakness. 02:00 This is a distal predominant muscular dystrophy and so the symptoms are distal. 02:04 We see distal upper extremity and lower extremity weakness and atrophy. 02:09 You can see here in the picture to the far right, this patient has a atrophic distal muscles in the upper extremity both arms symmetrically and bilaterally as well as in the ankles with prominent atrophy of the calves. 02:22 Importantly, we can see other symptoms in these conditions. 02:25 Patients may have mental retardation, reduced gray and white matter within the brain that contribute to that cognitive dysfunction, frontal balding is a prominent finding. 02:35 And you can see that a little bit in the picture here with a prominent forehead. 02:39 Temporal wasting or loss of muscle along the bilateral aspect of the face can result in a thin appearing face that often is pointed. 02:48 And that gives the face a hatchet appearance and that's been termed in the literature, a hatchet face. 02:54 Entosis as a result of the bifacial weakness. 02:57 So some characteristic findings that make this condition very different on exam and at presentation than some of the other muscular dystrophies. 03:06 In addition, patients may have early cataracts and that's important to screen for. 03:10 This condition affects cardiac conduction and we can see cardiac conduction abnormalities in patients who have those abnormalities may need screening and early pacemaker placement. 03:20 This is very important for managing a potential life ending complication. 03:25 And that said through cardiomyopathy. 03:27 We can see endocrine abnormalities hypogonadism, pituitary dysfunction as a result of this condition, which really affects function across the whole body and respiratory muscle weakness and dysfunction. 03:38 Hypoventilation or obesity hypoventilation can be a significant symptom that also needs to be screened and managed. 03:46 What about Myotonic Dystrophy Type II? How does that differ in its clinical presentation from Myotonic Dystrophy Type I? Well, again, this is a repeat disorder here not a trinucleotide repeat disorder. 03:59 This is a CCTG repeat condition. 04:03 It's prevalent in European predominant families and inheritance patterns so European predominant disease. 04:10 Here we see distal arm and proximal leg weakness which makes it different from DM1. 04:16 In addition, we also see calf hypertrophy. 04:19 Again from fibrosis and scarring within the distal muscles as well as myaiglas and you can see here in the picture how different this presentation is from DM1. 04:29 We saw thin distal upper extremities and thin calf muscles in DM1. 04:34 Here we see thin, upper extremities the forearms of the upper extremity but calf pseudohypertrophy is prominent and there is proximal lower extremity weakness which differs from DM1. 04:46 Often without cognitive dysfunction, which can be seen in DM1 and we do see associations with cataracts and cardiomyopathy in patients with DM2 which is important for screening and longitudinal management of these patients. 05:00 So DM1 and DM2 are the two most important distal muscular dystrophies to consider but we do see others. 05:07 And for these, I just want you to know the names. 05:09 These result in dysfunction of other proteins that are involved in that anchoring of the of the circle glycan complex in the muscle. 05:18 We see Welander's, which is really an extensive weakness. 05:22 There's problems with distal extensor muscles. 05:26 Dysferlinopathies are a common group of distal predominant muscular dystrophies. 05:31 Myofibrillar myopathy, which we'll talk about in a subsequent lecture. 05:35 And then there's some non muscular dystrophies which is the hereditary or inherited inclusion body myositis would be the most prototypical, non muscular dystrophy cause of inherited distal weakness and that's hereditary inclusion body myositis.
About the Lecture
The lecture Distal Predominant Muscular Dystrophies by Roy Strowd, MD is from the course Hereditary Neuromuscular Disorders.
Included Quiz Questions
With regard to type I myotonic dystrophy, which of the follow statements is most accurate?
- Ocular and cardiac screening are important in the treatment of these patients.
- It is inherited in an X-linked dominant manner.
- Facial muscles are normally spared.
- Patients typically have normal cognitive function.
- Proximal muscle involvement is more common than distal muscle involvement.
With regard to type II myotonic dystrophy, which of the follow statements is most accurate?
- Patients can have calf hypertrophy.
- It is caused by a trinucleotide repeat error.
- It is common in the Asian population.
- It is associated with cognitive impairment and balding.
- The distal muscles are more involved than the proximal muscles.
Which of the following is a proximal-dominant myotonic dystrophy?
- DM2
- Welander’s
- Dysferlinopathies
- Myofibrillary myopathy
- Inclusion-body myositis
Author of lecture Distal Predominant Muscular Dystrophies

Roy Strowd, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
