Playlist
Show Playlist
Hide Playlist
Congenital Hypertrophic Pyloric Stenosis

-
Slides Structural GI Diseases.pdf
-
Download Lecture Overview
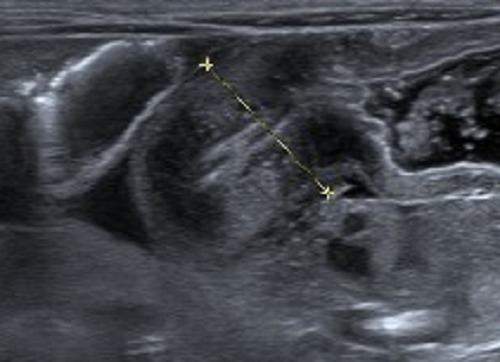
00:02 In this lecture, we’re going to discuss structural gastro and intestinal diseases in children. 00:07 Specifically, ones involving the enteric system. 00:11 Let’s start with congenital hypertrophic pyloric stenosis. 00:16 So here’s a case for you. 00:18 A baby who’s a male who is four weeks old and is born to a P1G1 mother. 00:24 In other words, it’s her first pregnancy and first child, presents to the emergency department with new onset projectile nonbilious vomiting after feeding. 00:34 Physical exam reveals a firm, olive-shaped abdominal mass. 00:38 So new onset projectile nonbilious vomiting after feeding, firm, olive-shaped abdominal mass in a first time mother. 00:48 This is a classic case of pyloric stenosis. 00:54 So pyloric stenosis is a hypertrophy of the pylorus muscle, resulting in a gastric outlet obstruction. 01:01 This happens typically in about one to three out of every thousand live births. 01:06 As a pediatrician, we see this fairly frequently. 01:10 It’s multifactorial. 01:13 Risk factors include being a first born male, which is fully one-third cases, having a family history of pyloric stenosis, but also macrolide antibiotic use in the first two weeks of life increases the risk of pyloric stenosis. 01:30 So it has both genetic and environmental causes, none of which are fully understood. 01:36 Typically, these patients will present with nonbilious because the constriction is before the outlet of the gallbladder. 01:44 It’s projectile because the stomach contents are under quite a bit of pressure and will literally fly out of the child’s mouth, and it’s usually postprandial. 01:53 They eat and then they immediately vomit. 01:56 And usually, they’re hungry again after they vomit. 01:59 You may palpate an olive-like mass in the right upper quadrant. 02:04 That is a very high-yield test question. 02:09 But the fact that that’s a high-yield test question is a little bit absurd because in reality, we almost never actually feel the olive-like mass. 02:17 I felt it myself once in patient with a ventral hernia, but other than that, I’ve never appreciated the mass. 02:23 Nonetheless, it’s common on test questions. 02:26 What you might see in a patient if you were to offer that child formula or Pedialyte, as their child is trying to eat, is you might appreciate peristaltic waves proceeding through the stomach as that child is trying to digest the food. 02:44 Children will get dehydrated quickly because they’re really not capable of keeping anything down. 02:49 And they may have worsened jaundice simply because of inability to pass stool because of a lack of food. 02:57 On this slide, you can see a very severe case, on the very right side of the slide. 03:03 Here, you can see the palpable mass in this child’s abdomen and distended belly. 03:08 This child has been having pyloric stenosis for a long time and this is really a misdiagnosis. 03:16 One thing that’s key that you’ll notice that is unique to pyloric stenosis is you will see a hypochloremic metabolic alkalosis. 03:25 These children will have a low chloride because they have been vomiting up their hydrochloric acid that the stomach makes. 03:32 And that’s also why they’re alkalotic. 03:35 They will also have a resultant hypokalemia. 03:40 So if you suspect pyloric stenosis, the test of choice is the ultrasound. 03:46 It’s a simple expedient test where the probe is placed just over the outlet of the stomach and a thickened pylorus is measured. 03:56 If we have a patient with pyloric stenosis, the first step is to stabilize the child. 04:00 So certainly if a child is having alkalosis, we want to correct that. 04:04 Usually simple hydration is sufficient. 04:07 Then, the patient in the United States is typically taken for a pyloromyotomy. 04:12 This is a very quick and relatively simple and safe procedure where surgeons make a longitudinal incision through the pylorus to the outer layer of the submucosa. 04:23 They don’t cut directly through the full wall of the mucosa, simply through the muscular layer on the outside of it. 04:30 That loosens things up and allows the food to pass through. 04:34 They can do this laparoscopically. 04:37 And after the procedure, they then will proceed to reinitiate feeding, generally 12 or 24 hours later and see how things go. 04:46 Usually, children eat just fine afterwards and have a great outcome. 04:50 In some parts of the world, instead of doing a pyloromyotomy, they will simply advance a tube and feed the child postpylorically. 04:59 This is somewhat controversial. 05:02 Most time in the US, the surgeons prefer to do pyloromyotomy because the child is not n.p.o. for any period of time. 05:09 Remember, if a child’s made n.p.o., they may have feeding difficulties later. 05:14 Additionally, in the hands of experienced surgeons, this is an extraordinarily safe procedure.
About the Lecture
The lecture Congenital Hypertrophic Pyloric Stenosis by Brian Alverson, MD is from the course Pediatric Gastroenterology.
Included Quiz Questions
What is a risk factor for infantile hypertrophic pyloric stenosis?
- Early use of erythromycin
- Female gender
- Second child in family
- Bilious emesis
- Diarrhea
Which of the following acid-base disorders is typically seen in infants with hypertrophic pyloric stenosis?
- Hypochloremic metabolic alkalosis
- High anion gap metabolic acidosis
- Respiratory acidosis
- Non-anion gap metabolic acidosis
- Respiratory alkalosis
Which of the following is a characteristic physical examination finding in a 4-week-old infant with nonbilious and forceful vomiting and a history of erythromycin use 3 weeks ago?
- Olive-shaped mass in the right upper quadrant
- Circular mass in the left upper quadrant
- Linear mass in the epigastrium
- Firm mass near the left margin of the rectus abdominis
- Soft mass near the right margin of the rectus abdominis
Author of lecture Congenital Hypertrophic Pyloric Stenosis

Brian Alverson, MD
Customer reviews
4,5 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
1 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
I like the explanation of the surgical and non-surgical treatments
Good summary of the disease. Easy to remember. Good to have the risk-factors! Thank you!
