Playlist
Show Playlist
Hide Playlist
Chronic Pancreatitis with Case

-
Slides Gastroenterology 18 Pancreas Disorders.pdf
-
Reference List Gastroenterology.pdf
-
Download Lecture Overview
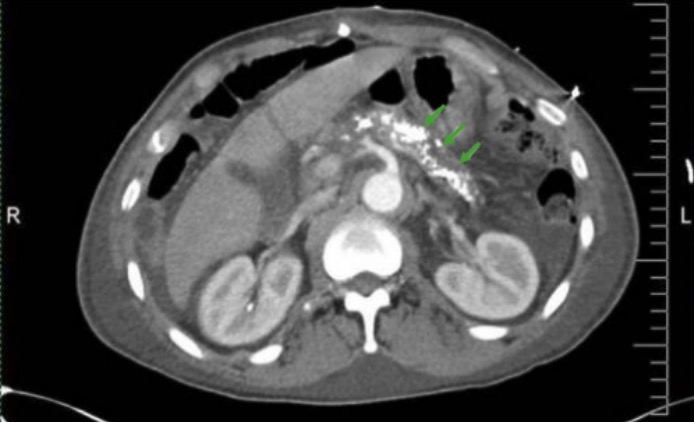
00:01 Let's move on to our next case. 00:04 A 68-year-old woman with a history of alcohol use disorder is seen in clinic for two years of chronic diarrhea. 00:11 She has two to three loose, foul smelling bowel movements daily and intermittent epigastric pain after eating. 00:19 She has lost 10 kg in the past year. 00:22 She quit drinking two years ago, smokes one pack per day and is not on any medications. 00:27 Vitals are normal. 00:29 On exam, she has temporal wasting and mild epigastric tenderness without rebound or guarding. 00:35 There is no hepatosplenomegaly and no jaundice. 00:38 Labs show a serum lipase of 33. 00:42 And abdominal ultrasound shows pancreatic calcifications but no masses. 00:47 So we are asked, what is the best next step in management? So let's point out some key features. 00:54 She has chronic diarrhea with epigastric pain which would prompt you to think of perhaps a malabsorption syndrome. 01:01 In addition, she does have heavy alcohol use and a history of smoking. 01:07 And on exam, she has exam findings that support malnutrition. 01:13 Her normal lipase and pancreatic calcifications may also be helpful in our diagnosis. 01:20 So, let's now talk about chronic pancreatitis. 01:25 To understand how chronic pancreatitis forms, we have to go back to the physiology of the pancreas and what its role is in digesting food. 01:34 So the pancreas has two functions. 01:36 It has an endocrine function and it has an exocrine gland function. 01:40 The endocrine gland function involves secreting insulin, glucagon and somatostatin to aid in the regulation of blood sugar. 01:48 On the other hand, the exocrine function involves producing pancreatic enzymes like protease, lipase and amylase that all help with digestion of food. 01:59 So, in chronic pancreatitis, patients have multiple bouts of inflammation that then leads to irreversible injury and then fibrosis of the pancreas. 02:11 So symptoms include, having intermittent abdominal pain often radiating to the back. 02:16 They may present with diarrhea and steatorrhea, so fatty stools, and they may have weight loss. 02:24 And all of this is related to the inability to process the food that we -- that ordinarily the pancreas would allow us to digest. 02:32 So patients may often present also with diabetes due to the loss of the endocrine function of the pancreas. 02:40 And because they're unable to process fats, they may also have fat soluble vitamin deficiencies. 02:47 Common causes of chronic pancreatitis include alcohol use and anything that causes recurrent bouts of pancreatitis. 02:57 The diagnosis can be quite difficult to make. 03:01 This is because on labs, amylase and lipase are often normal. 03:06 In addition, on imaging, you might find pancreatic calcifications as shown here on the CT scan showing bright white calcifications within the pancreas. 03:18 However, you may not see this finding, so you cannot base your diagnosis on this. 03:24 MRCP or endoscopic ultrasound may help you look for abnormalities in the pancreatic duct. 03:31 But again, not always done. 03:33 And if you suspect malabsorption, you could do 72 hour fecal fat testing. 03:39 In the end, it is mostly a clinical diagnosis and we manage it with pain control, reducing any triggers that are known to cause pancreatitis. 03:51 So, cutting back on alcohol and smoking cessation and replacing the pancreatic enzymes that the person can no longer secrete. So now let's go back to our case. 04:04 We had a 68-year-old woman with chronic diarrhea and epigastric pain. 04:09 She has a history of heavy alcohol use and smoking which are both risk factors for chronic pancreatitis. 04:17 She has evidence of malnutrition and now we know that a normal lipase can be found in chronic pancreatitis as are the pancreatic calcifications seen on her imaging. 04:27 So, the best next step in management would be to screen for fat soluble vitamin deficiencies since she is at high risk for this, offering pain control. 04:37 And of course, counseling her on smoking cessation and replacing her pancreatic enzymes.
About the Lecture
The lecture Chronic Pancreatitis with Case by Kelley Chuang, MD is from the course Disorders of the Pancreas.
Included Quiz Questions
Which of the following is a possible risk factor for chronic pancreatitis?
- Alcohol
- Anorexia
- High-fiber diet
- Hypocalcemia
- Hypokalemia
Which of the following is the treatment of choice for chronic pancreatitis?
- Pain control and pancreatic enzyme replacement
- Surgery
- Antibiotics
- Proton pump inhibitors
- Laxatives
Author of lecture Chronic Pancreatitis with Case

Kelley Chuang, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
All of her lectures are clear and concise, and the cases allow us to come up with our own answer before she explains them.
