Playlist
Show Playlist
Hide Playlist
Cervical Spine: Introduction

-
Slides Osteopathic Diagnosis of the Cervical Region.pdf
-
Reference List Osteopathic Manipulative Medicine.pdf
-
Download Lecture Overview
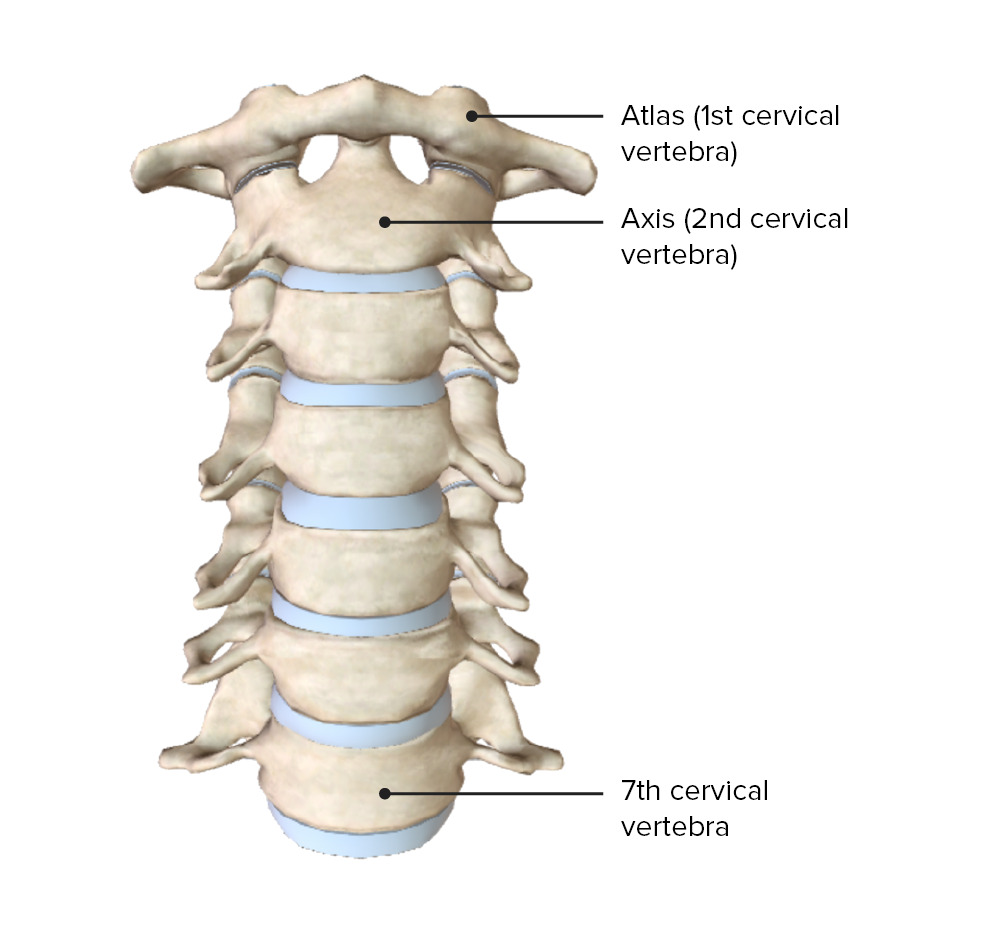
00:01 So let's review the cervical spine Here we have the 7 cervical vertebrae and from C3 to C7, we consider these the typical vertebrae They're typical because they have similar structures to the thoracic and lumbar spine. 00:15 The two atypical vertebrae is C1 and C2. 00:19 The C0 and C1 articulation is the articulation of the skull or the occiput and there's 2 condyles in the occiput articulating with C1 and this is important because that's where your skull will rest upon your neck. 00:34 So here is a superior view and here you could see how the Atlas has two superior articular facets where the occiput, the condyles of the occiput kinda sit on top of that superior articular facet. 00:46 Here you could also note the dens which comes up superiorly from the access. 00:49 The dens held tightly by ligaments. 00:53 The transverse ligament posteriorly and the alar ligament anteriorly. 00:57 There's also a posterior and anterior arch as opposed to a typical vertebral body. 01:04 Here is an image of C2 or the axis. 01:07 and with the axis here, you could see the dens as the dens comes up and protrudes through the atlas and you also have here more of a spinous process and the lamina compared to the axis at the atlas. 01:22 Here's a lateral view of the axis. 01:24 You could see how the dens comes up and protrudes through the atlas. 01:27 There's also a little bit more of a vertebral body to the segment. 01:33 C3 to C7 is considered your typical cervical vertebrae. 01:38 Generally it has a body, 2 pedicles, 2 laminae and 1 spinous process. 01:45 There's also 2 articular pillars, so the articular pillars are more posterior than the transverse processes. 01:51 These are the points that are utilized when you're palpating ang trying to diagnose any sort of asymmetry in the cervical spine. 02:00 So there are ligaments that run along the cervical vertebrae. 02:03 They're anterior longitudinal ligament and posterior longitudinal ligament come up and attach to the occiput. 02:10 You have your ligamentum flavum which runs between the cervical segments and there's other ligaments that help to maintain the structure of the cervical spine. 02:21 Your OA articulation is mostly responsible for flexion and extension of the cervical spine. 02:30 The head when it goes into flexion, the condyles will glide posteriorly and when the head goes into extension, the occipital condyles will glide anteriorly. 02:38 This is different from the rest of the spine. 02:42 So the motion at the OA junction is primarily flexion and extension and there's a small component of side bending. 02:50 Usually when there is a somatic dysfunction present, the flexion and extension component is significant and you have rotation and side bending coupled in opposite directions because of the anatomical structure of the region. 03:04 It's almost as you have to think of the skull or sphere gliding on the neck or stick. 03:11 And so the motion there, because of the condyles being pointed anteriorly and superiorly, it's gonna create certain motions creating that rotation and side bending similar to Type 1 dysfunctions of the thoracic and lumbar spine. 03:27 At the AA joint of C1-C2 articulation, the motion is primarily rotation. 03:33 Ligaments that hold the dens in place prevent really other motions such as flexion and extension. 03:40 Dysfunctions in this region really is only in rotation. 03:47 For C3 to C7, these are typical vertebrae. 03:51 The facet orientation is more of a transverse plane so a lot more rotation in the region The facets help to guide motion but the limitations of motion is really through ligaments and muscles. 04:05 Uncate processes sometimes could form along the body which usually occurs through degeneration. 04:14 So C3 to C7 are your typical vertebrae and they do have intervertebral disc These disc do have pressure upon them and the pressure does increase when you lean forward and when you're sitting. 04:29 And so, these forces compress on the disc and if you think about the head really is almost like a bowling ball in weight, 10 lbs., and your neck being a thin stick. 04:40 So any sort of forward bending or flexion, any slouching will put a lot of pressure on the neck and cause, could potentially cause problems and issues. 04:49 C3 to C7 are your typical cervical vertebrae. 04:52 These segments follows Fryettes principles for type II somatic dysfuction Fryettes principles applies to thoracic and lumbar spine biomechanics. 05:01 So we are gonna further discuss that in our thoracic's lecture. 05:04 But what it really says is that in a single segment dysfunction, there is a flexion and extension component. 05:12 So it is a non-neutral segment. 05:14 And so our cervical spine act in a similar fashion They act as an individual segment and there are certain motions that are coupled with it. 05:21 So whenever you rotate and side bend a cervical segment, it is always gonna be in the same direction for C3 to C7. 05:30 The vertebrobasilar artery system This system is really important when talking about evaluation of the cervical spine. 05:37 It is important to keep in mind the anatomy of this vessel because it could traverse the cervical spine through the transverse processes and because of how it courses through the cervical spine, certain motions could limit the blood flow and could also put the blood vessel at risk. 05:54 And so, the vertebral arteries come off the subclavian artery and then enter the transverse processes usually at the level of C6 and 7.5% of the cases could enter at the level of C7 It does preceeds superiorly then through the transverse processe up to C1. 06:12 At C1 what happens, it travels across the posterior arch of the atlas and then enters the foramen of magnum. 06:18 So it almost makes a 90 degree turn and then comes up. 06:22 So inside the skull, the vertebral artery then joins and forms the basal artery. 06:28 Sometimes when you have overextension or too much side bending rotation, it could actually compress that verteral artery and put the blood flow to head at risk. 06:37 So, it is really important to understand how the anatomy of that blood vessel could potentially affect blood flow to the head. 06:46 Looking at the muscles of the cervical spine, in general, there are a lot more thicker, heavier muscles in the posterior aspect of the neck than the anterior portion of the neck. 06:56 So, our neck resist forward flexion a lot more than extension. 07:01 So a lot of times we could have an imbalance of the neck muscles and that could cause problems in somatic dysfunctions. 07:08 So the superficial muscles in the posterior aspect of the neck start with the trapezius, erector spinae muscles, that's a continuation from the thoracic and lumbar spine. 07:21 More intermediate muscles could be noted here in terms of the splenius cervicis and capitis And you have these deep posterior neck muscles, these muscles tend to be more of a factor in contributing to type II somatic dysfunctions in the neck. 07:38 This includes the rectus capitis, posterior major and minor, obliquus and the interspinales and intertransversii. 07:48 There are some anterior muscles that attach to the deep portion of the cervical spine. 07:55 And so these you could note how one's anteriorly and again a lot thinner, not as strong.
About the Lecture
The lecture Cervical Spine: Introduction by Sheldon C. Yao, DO is from the course Osteopathic Diagnosis of the Cervical Region. It contains the following chapters:
- Cervical Spine
- C0–C1 Articulation (OA)
- C1–C2 Articulation (AA)
Included Quiz Questions
Which of the following cervical vertebrae is also known as the atlas?
- C1
- C2
- C3
- C4
- C5
Which of the following cervical vertebrae is also known as the axis?
- C2
- C3
- C4
- C5
- C1
Which of the following motions is the primary motion of the C0 (occiput) and C1 articulation?
- Flexion and extension
- Flexion only
- Sidebending
- Torsion
- Rotation
Which of the following motions is the primary motion of the C1 and C2 articulation?
- Rotation
- Flexion
- Extension
- Sidebending
- Torsion
From which of the following vessels do the vertebral arteries arise?
- Subclavian
- Internal jugular
- Internal carotid
- External carotid
- External jugular
Author of lecture Cervical Spine: Introduction

Sheldon C. Yao, DO
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
