Playlist
Show Playlist
Hide Playlist
Case: 53-year-old Man with Generalized Weakness

-
Slides Diseases of the Motor Neurons.pdf
-
Download Lecture Overview
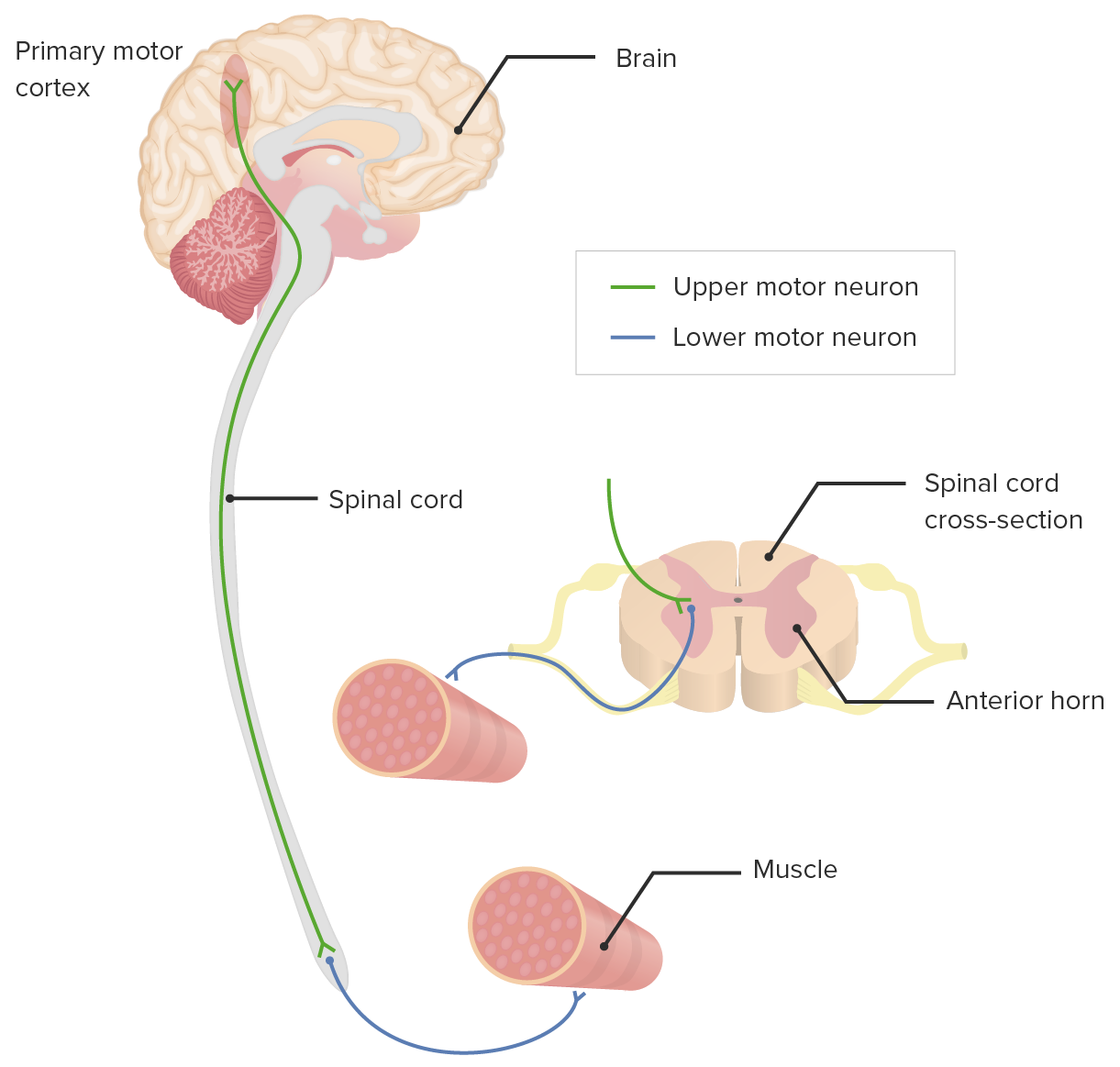
00:01 So now let's turn to a case and think a little bit more about the presentation, diagnosis and management of patients with motor neuron disease and focus specifically on one of the most common types of motor neuron disease. 00:13 This a 53 year old otherwise healthy construction worker who presents on referral from his primary physician for complaints of generalized weakness and clumsiness. 00:22 He reports that for the past several months, he has found his job more and more difficult to complete due to weakness. 00:29 He's finally seeking evaluation so that he continue his work. 00:32 Examination reveals weakness of all the extremities with atrophy of the intrinsic hand muscles with occasional fasciculations of the first dorsal interosseous muscle. 00:42 Reflexes are hypoactive in the upper extremities and hyperactive in the lower extremities. 00:48 Tone in the lower extremities is increased. 00:49 Cranial nerves and sensory examinations are entirely normal. 00:53 So a few things we're seeing that are important in this case, one is the distribution. 00:58 We see that all extremities are involved, there's both lower and upper motor neuron findings. 01:03 The lower motor neuron findings are primarily in the arms and the upper motor neuron findings are below the arms and there's that suggestion of this combined upper and lower motor neuron pathology, suggesting either cervical spine disease or motor neuron disease. 01:18 Reflexes show again hypoactive reflexes in the upper extremities and hyperactive in the lower extremities And we see normal sensory examination. 01:26 This is fitting the picture of a motor neuron disorder or its mimic. 01:32 And importantly, in terms of wildcards, this is an otherwise healthy individual. 01:35 He's a construction worker, and we need to think about that but no other clear underlying historical details that suggest an alternative etiology. 01:45 So what's the diagnosis? Is this ALS, B12 deficiency, cervical spinal cord disease or a paraneoplastic myelitis? Well, all of these probably need to be evaluated in this patient. 01:57 Vitamin B12 deficiency can present with a myeloneuropathy, so a cervical or a myelopathy, a spinal cord disease in addition to neuropathy, presence of lower nerve dysfunction, peripheral nervous system dysfunction, and can be evaluated with a B12 level. 02:14 Typically, we do see patients present with some sensory findings, but a B12 check is important for this patient but unlikely to be the ultimate diagnosis. 02:22 Cervical spine disease could present as this and the presentation is not inconsistent with this disorder. 02:28 But the presence of that combination of upper and lower motor neuron findings in this short period of time requires evaluation for a motor neuron disease. 02:38 Paraneoplastic myelitis can also present in this way, the patient does not have a history of cancer. 02:43 But importantly, neurologic symptoms can predate the diagnosis of cancer and so this is unlikely the etiology for this patient. 02:51 We need to think about a motor neuron disease but evaluation of potential paraneoplastic causes is important in this patient. 02:58 And ultimately, this patient was diagnosed with a motor neuron disease. 03:02 The classic motor neuron disease being amyotrophic lateral sclerosis also called Lou Gehrig's disease. 03:08 And this classically presents with upper and lower motor neuron findings, often overlapping in the same spinal levels with at least three spinal levels being involved - the cervical, thoracic, lumbosacral, brainstem or brain
About the Lecture
The lecture Case: 53-year-old Man with Generalized Weakness by Roy Strowd, MD is from the course Diseases of the Motor Neurons.
Included Quiz Questions
Which motor neuron lesion is paired correctly with its clinical finding?
- Upper motor neuron ‒ spasticity
- Lower motor neuron ‒ hyperreflexia
- Lower motor neuron ‒ pseudohypertrophy
- Upper motor neuron ‒ fasciculations
- Upper motor neuron ‒ atrophy
ALS is most commonly associated with which pattern of clinical findings?
- Both UMN and LMN symptoms, normal sensory exam, and abnormal electrodiagnostic studies
- LMN symptoms only, unilateral lower extremity pain, and abnormal electrodiagnostic studies
- UMN symptoms only, normal sensory exam, and normal electrodiagnostic studies
- Both UMN and LMN symptoms, stocking-glove pattern of sensory loss, and abnormal electrodiagnostic studies
- UMN symptoms in the arms, LMN symptoms in the legs, and hyperreflexia
Author of lecture Case: 53-year-old Man with Generalized Weakness

Roy Strowd, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
