Playlist
Show Playlist
Hide Playlist
Case: 45-year-old Man with Lower Extremity Weakness

-
Slides Diseases of the Spinal Cord.pdf
-
Download Lecture Overview
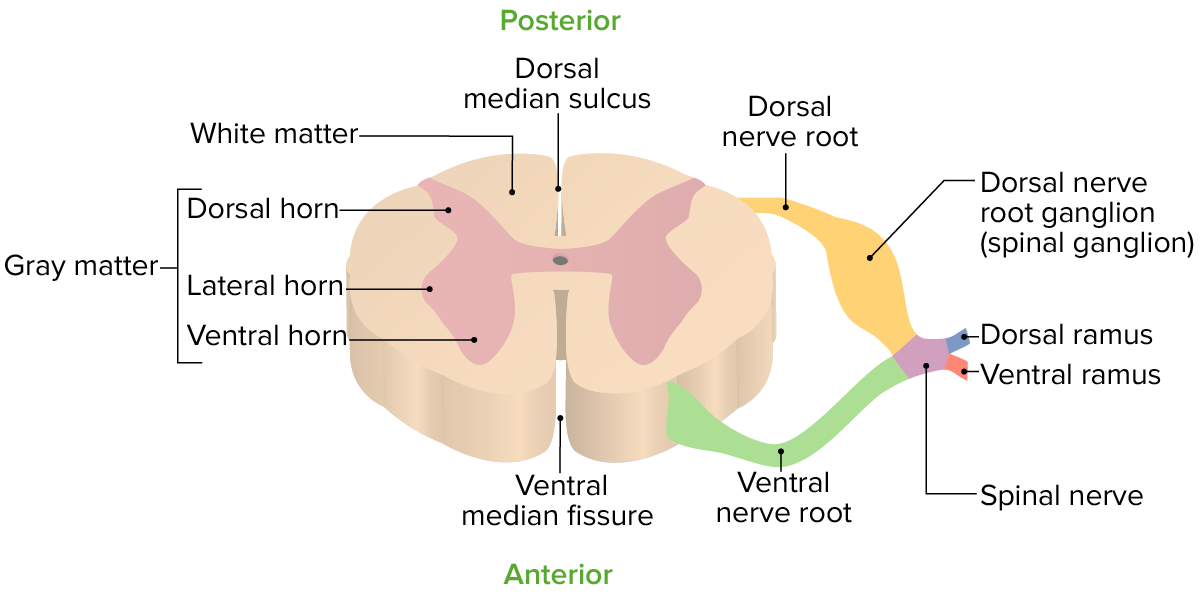
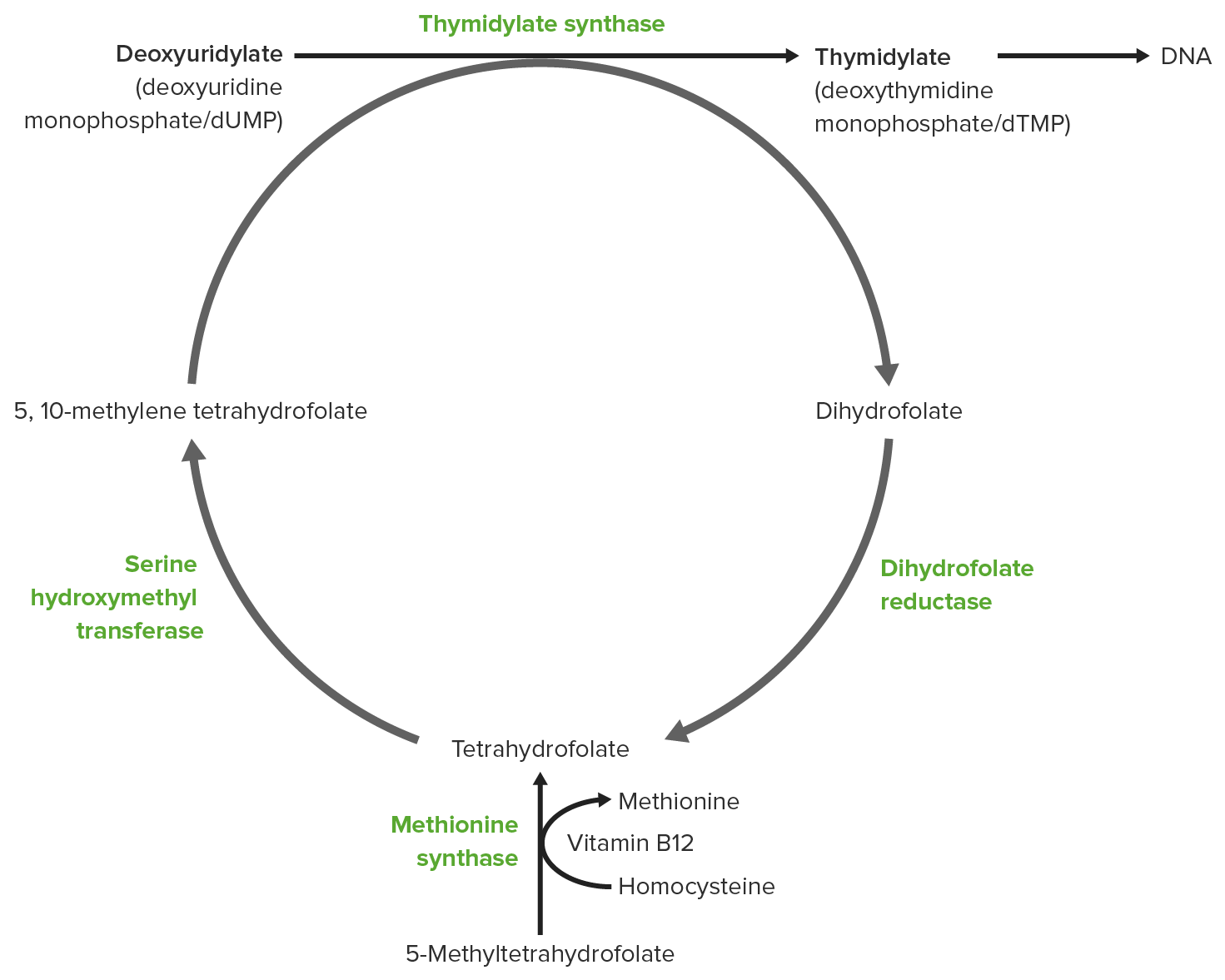
00:00 In this talk, we will review the toxic and metabolic myelopathies. Let's start with a case. This is a 45-year-old man who presents with weakness in the legs. 00:13 The patient first developed heaviness and weakness of his legs starting 2 months ago. 00:18 Both legs have been affected. He reports difficulty with balance and ambulation. 00:24 He was using a cane and is now using a walker for ambulation. He reports numbness and tingling in the legs bilaterally as well as in his hands. There are no symptoms in his face. Neurologic exam shows mild memory loss with 3/3 immediate registration and 1/3 recall at 5 minutes. Attention is slightly reduced. Strength examination shows a paraparesis with 4/5 strength in the bilateral lower extremities. There is reduced vibration and proprioception in the legs bilaterally, but intact pain and temperature sensation. Deep tendon reflexes are 3+ in the bilateral legs and arms. 01:10 So there are a number of key features that we can hone in on in this case. 01:14 This patient has a paraparesis, symptoms affecting the legs, to some degree the arms and sparing the face or cranial nerves. This points to a disorder in the spinal cord. In addition, there is a unique combination of symptoms and white matter tracts that appear to be affected. The patient has motor weakness likely affecting the corticospinal tract and reduced vibration proprioception affecting the dorsal columns. Importantly, we see that the anterolateral system is preserved and this supports the diagnosis of a myelopathy. Here, we can see the imaging that was performed in this patient and we see very characteristic abnormalities for this type of condition. You can see most of the cord appears normal; however, there is this increased T2 hyperintensity primarily restricted to the dorsal columns, what has been termed the inverted V sign. So, what's the most likely diagnosis? Is this multiple sclerosis, a spinal cord astrocytoma, lymphomatous meningitis, or vitamin B12 deficiency. Well, this is not the typical presentation or imaging findings for multiple sclerosis. The patient does have a subacute and progressive course, but imaging is inconsistent with an inflammatory disorder like multiple sclerosis. This is not the diagnosis of spinal cord astrocytoma. There is no cord swelling or edema that would be expected from a spinal cord tumor. And imaging findings are restricted to the white matter tracts in the dorsal column, which is more typically seen with a metabolic etiology and not a spinal cord tumor. This is not the presentation of lymphomatous meningitis. There is no history of cancer and these intramedullary changes don't suggest a leptomeningeal process. 03:11 This is the typical presentation of vitamin B12 deficiency and a disorder that has been termed subacute combined degeneration. This is one of the most common and well-known toxic or metabolic causes of myelopathy.
About the Lecture
The lecture Case: 45-year-old Man with Lower Extremity Weakness by Roy Strowd, MD is from the course Diseases of the Spinal Cord.
Included Quiz Questions
What is one of the most common toxic/metabolic causes of myelopathy?
- Vitamin B12 deficiency
- Vitamin B6 deficiency
- Vitamin C deficiency
- Lead poisoning
- Lupus meningitis
Which ascending pathways are affected by vitamin B12 deficiency?
- Dorsal columns
- Anterolateral tracts
- Spinothalamic tracts
- Corticospinal tracts
- Tectospinal tracts
Author of lecture Case: 45-year-old Man with Lower Extremity Weakness

Roy Strowd, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
