Playlist
Show Playlist
Hide Playlist
Lesions and Diseases of the Spinal Cord: Brown-Séquard Syndrome and Tabes Dorsalis

-
Slides 5 SpinalCord3 BrainAndNervousSystem.pdf
-
Reference List Anatomy.pdf
-
Download Lecture Overview
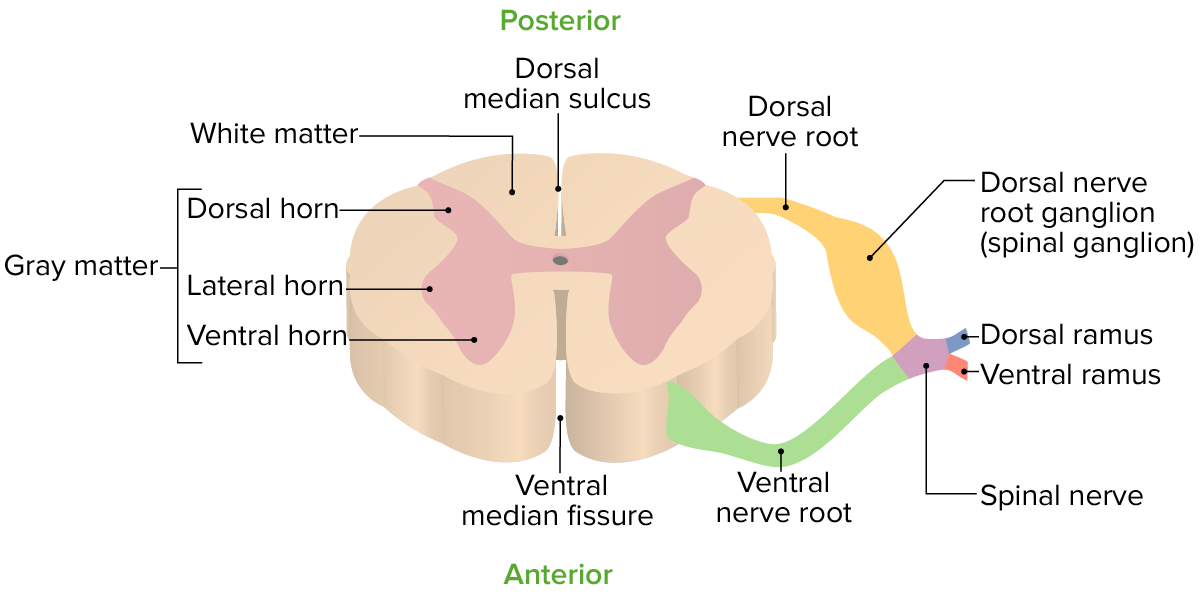
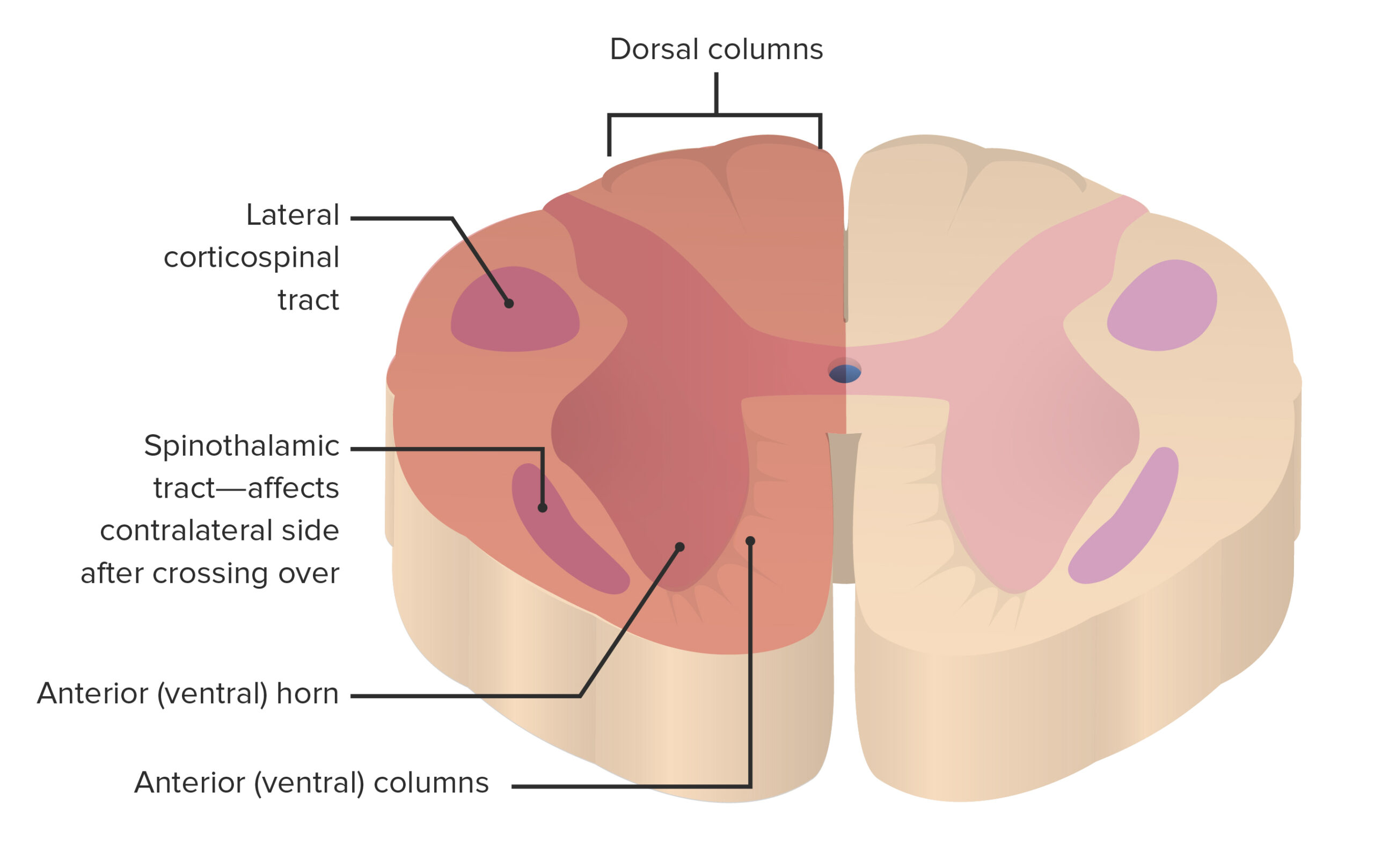
00:00 Welcome to this lecture on the spinal cord. 00:06 Our first slide depicts a lesion of the spinal cord. 00:10 This lesion is involving the dorsal columns/medial lemniscal system. 00:18 The lesion at this level within the spinal cord is affecting the first order neurons as they ascend and this lesion then is ipsilateral and as a result to this lesion being on the ipsilateral side of the pathway, there will be an ipsilateral loss of function below this level of the lesion. 00:41 The loss of function would involve the loss of fine touch, two-point discrimination, loss of pressure and vibration senses, as well as conscious proprioception as these are the normal functions that are conveyed by this ascending pathway. 01:02 Here, you’re looking at a cross-section through the spinal cord. 01:07 And the lesion is depicted over here in the shaded light green area. 01:13 And so if we identify the lesion and the accompanying clinical features, the lesion that’s a hemisection of the spinal cord as you see here is referred to as Brown-Séquard Syndrome. 01:27 Brown-Séquard Syndrome is gonna involve various aspects of the spinal cord, the dorsal columns would be involved in through here. 01:38 So again, this will be ipsilateral loss of fine structure, two-point discrimination, vibration, pressure, and conscious proprioception at and below that particular level of the lesion. 01:54 The spinothalamic tracts are also involved here and in this case, there will be a contralateral loss of pain and temperature 1-2 segments below the lesion, and the reason that the loss of pain and temperature is 1-2 segments below the lesion is due to Lissauer’s tract. 02:22 Lissauer’s tract, when the neurons, or at this level are ascending a couple of levels, and so this is involving those levels that are below this particular level in the spinal cord. 02:36 Please note specifically that at level of the lesion, there is complete ipsilateral loss of all sensations. 02:45 Lastly, the corticospinal tracts are involved. 02:51 and at this particular level, there will be an ipsilateral paresis at and below the lesion. 03:00 Here, we’re looking at a continuation of Brown-Séquard Syndrome. 03:07 In addition, to what we saw in the previous slide, descending hypothalamics will be lesioned. 03:15 And so we lose the descending hypothalamic output. 03:18 And at this lesion is above spinal cord level T1. 03:23 The loss of sympathetics will result in ipsilateral Horner’s Syndrome. 03:29 So, miosis, anhidrosis, and ptosis would be the triad of symptoms associated classically with Horner’s Syndrome. 03:42 Lower motor neurons would be involved here. 03:47 They would be damaged in the dorsal grey horn area and as a result there will be flaccid paralysis at the level of the lesion. 04:00 And as it’s shown here, with paralysis, loss of muscle tone, and just a general state of hypotonia. 04:09 Here, we’re looking at again a cross-section of the spinal cord but this is a different lesion, or have a different set of clinical features. 04:25 Here, the lesion is, in this area of the cord, the posterior part. 04:30 So it’s involving the dorsal columns. 04:35 This particular lesion is referred to as Tabes Dorsalis. 04:42 And this disease is characterized by a slow degeneration, demyelination of nerves found primarily in these dorsal columns. 04:53 So, you have the fasciculus gracilis and the fasciculus cuneatus ascending through this area of the spinal cord. 05:03 What are the accompanying clinical features of tabes dorsalis? Individuals that have this lesion complain of intense pain. 05:17 They complain of disturbed sensation. 05:23 and then usual high step gait. 05:30 There gait it is unsteady and they will exhibit a positive Romberg’s sign, which is demonstrated by a loss of balance when the patient has their eyes closed. 05:50 And this will be due to a loss of proprioception. 05:55 Due to disruption of proprioception, patients also exhibit sensory ataxia. 06:02 Sensory ataxia is characterized by an unsteady, stomping gait. 06:07 This is exaggerated when the eyes are closed.
About the Lecture
The lecture Lesions and Diseases of the Spinal Cord: Brown-Séquard Syndrome and Tabes Dorsalis by Craig Canby, PhD is from the course Spinal Cord.
Included Quiz Questions
Which of the following symptoms of Brown-Séquard syndrome may be found on the ipsilateral side?
- Loss of fine touch and conscious proprioception below the level of the lesion
- Loss of pain sensation below the level of the lesion
- Loss of vibration and 2-point discrimination above the level of the lesion
- Loss of temperature sensation below the level of the lesion
- Motor deficits above the level of lesion
Which of the following sensations would be lost on the contralateral side in a case of hemisection of the spinal cord?
- Pain sensation 1–2 segments below the level of the lesion
- Temperature sensation 1–2 segments above the level of the lesion
- Motor deficits above the level of the lesion
- Fine touch sensation below the level of the lesion
- Crude touch sensation on both sides
Which of the following statements regarding the symptoms of Brown-Séquard syndrome is INCORRECT?
- Spastic paralysis at the level of the lesion occurs.
- Ipsilateral Horner’s syndrome occurs.
- Contralateral loss of pain and temperature occurs.
- Ipsilateral loss of touch and vibration occurs.
- Ipsilateral paresis at and below the level of the lesion occurs.
A patient presents with a high step and an unsteady gait and has a positive Romberg sign. What is the MOST likely etiology?
- Demyelination of the nerves primarily found in the dorsal column
- Degeneration of white matter in the brain
- Hemisection of the spinal cord
- Vitamin C deficiency
- Infection with Borrelia burgdorferi
Author of lecture Lesions and Diseases of the Spinal Cord: Brown-Séquard Syndrome and Tabes Dorsalis

Craig Canby, PhD
Customer reviews
3,5 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
1 |
| 1 Star |
|
0 |
excellent lecture. very clear explanation, with diagrams annotations. good memory aide.
I feel the anatomy lectures are rather "static" like simply reading the narrative or bulletin points to the audience. Instead, I think the anatomy lectures, especially as we are not learning by a cadaver to gain the tactile feedbacks, might be better designed in a more inviting/ interactive way. Bringing in more pathological relevance, e.g. showing schema/ video/ autopsy would be largely helpful. Or to the minimum, highlighting the knowledge of "high yield" and compare them on an anatomic picture/schema may also improve the learning experience of these topics. I like many Lecturio lectures nonetheless, but I think anatomy, and especially the neural anatomy lectures has a lot of space to improve in such way. Thanks.
