Playlist
Show Playlist
Hide Playlist
BK and JC Virus – Polyomaviruses

-
02-33 Polyomaviruses.pdf
-
Download Lecture Overview
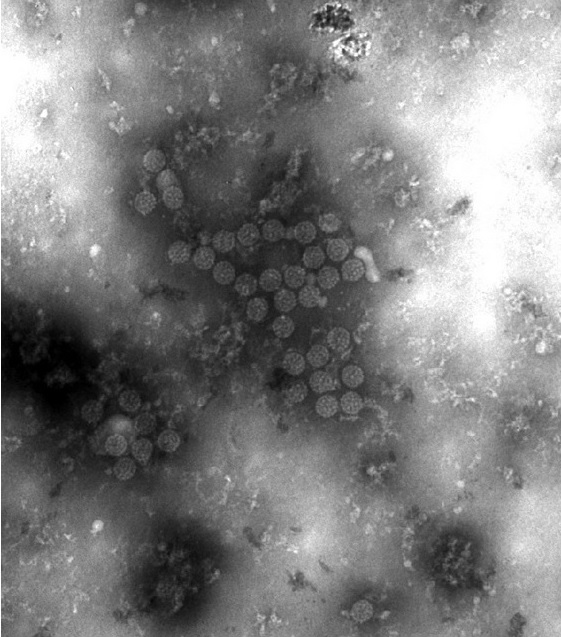
00:01 Polyomaviridae viruses. 00:04 The papillomaviruses are small and nonenveloped, with an icosahedral capsid, and, important to remember, circular, double-stranded DNA genome. 00:15 These are DNA viruses. 00:17 And you can see scanning electron microscopy of them on the right side of the slide. 00:22 These viruses are ubiquitous, but thankfully, they are very rarely pathogenic, and when so, it's typically in the setting of an immunosuppressive event. 00:32 There are 2 important or medically- relevant serotypes that we'll discuss today, the BK virus and JC virus. 00:41 Awfully unusual names for viruses, however, each of these viruses were named with the initials of the first patient ever described suffering from infection from those viruses. 00:53 Typical infection or pathogenesis with both viruses starts with a primary infection, which is completely asymptomatic, then latency occurs. 01:02 Immunosuppression, as I mentioned before, is the reason for allowing reactivation, and there's a cycle between reactivation and latency depending on the degree of immunosuppression. 01:14 In the case of JC virus, with reactivation after immunosuppression, viremia can occur, and the virus deposits in the central nervous system as a secondary site. 01:26 When it does so, then it causes leukoencephalopathy, and we'll talk about the clinical meaning of that in just a bit. 01:33 With the BK virus, reactivation occurring after immunosuppression allows the virus to target the kidney where it creates a urinary tract infection. 01:43 And, again, not the typical process as we would expect with a bacterial urinary tract infection, but something seen in the setting of immunosuppression in a kidney transplant recipient. 01:57 Who are the risks -- the people at risk for developing reactivation of either virus? These are especially our patients with immunodeficiencies caused by HIV infection, who would progress to AIDS. 02:10 Those who have received solid organ transplants, who are receiving immunosuppression to prevent rejection, and those patients with other underlying immunodeficiencies. 02:21 If we now look at the primary infections for these viruses, in general, the population at risk is all of us. 02:30 All of us, either are at risk for, or may already have acquired a very completely asymptomatic infection with either one or both of the viruses. 02:40 If we have any symptoms at all, they're incredibly mild. 02:43 A respiratory illness, very much like a common cold. 02:47 And since we rarely do further evaluation of a common cold, there would be no way to know that we had been infected with one or the other. 02:56 If we, then, look specifically at JC virus, this is the cause of progressive multifocal leukoencephalopathy, most often seen in patients who are immunocompromised due to HIV infection with AIDS. 03:09 Progressive multi-focal leukoencephalopathy, reactivation of the JC virus within the central nervous system creates a progressive impairment of speech, as well as vision, coordination through cerebellum dysfunction, as well as cognitive disarray. 03:25 Ultimately, this progresses to paralysis and death, very much like a very advanced or aggressive form of Alzheimer's syndrome. 03:33 This occurs because there are abnormal, targeted oligodendrocytes with reactivation of the virus that then cause the equivalent of demyelinating syndrome. 03:47 BK virus, again, occurs most often in renal or kidney transplant recipients, and this will be at some point after the primary transplant has occurred, typically, in the early, post-transplant period when immunosuppression is still quite extensive, and there's been time for the virus to reactivate within the renal setting itself. 04:08 These patients will have a severe urinary tract infection, not so much with dysurea, painful urination, but with a very extensive neutrophil response to these diseased reactivated cells. 04:22 So, one might see incredible leukocytosis or leukorrhea in the urine specimen, as well as viruria, which can be detected through sampling, and ultimately, kidney dysfunction. 04:37 The challenge is, that an reactivated BK virus, after a renal transplant, may manifest as transplant rejection. 04:45 In both cases, one we need to consider whether to increase or decrease the immunosuppression, hence, early diagnosis of BK virus is quite important. 04:56 So, ubiquitous viruses that most of us don't need to worry about, unless we practice either immunodeficiency medicine or transplant medicine, but when they occur, they need to be identified quickly. 05:08 Additional diseases are caused by more recently described Polyamide viruses are the Merkel cell carcinomas and the attractive dysplasia spine lesions. 05:18 Merkel cell carcinomas are caused by Merkel cell associated papillomavirus, which commonly colonizes the skin. 05:26 This is usually seen in older patients with light skin or type one or type two skin, and it usually occurs then on sun exposed skin. 05:36 So, a photosensitive injury caused by sun exposure. 05:41 The lesions themselves are rapidly growing firm, typically not tender, but they are shiny and a range of flesh colored to a bluish or even red appearance, color and appearance, and they create an intra cutaneous nodule. 05:57 These can be aggressive tumors, aggressive lesions with neuroendocrine involvement and malignancy. 06:04 As a subsequent extension, there is only a 50% five year survival. The typical dysplasia spine tolosa lesions caused by tricot dysplasia spending tolosa paloma virus. 06:17 These are seen almost exclusively in immunocompromised or immunosuppressed individuals. These lesions are flesh colored follicular papules, which typically are seen in the nose or forehead. 06:27 They can be associated with progressive hair loss, especially the eyebrows and eyelashes and even the scalp. 06:35 So a secondary alopecia. 06:37 Here we see a picture of a merkel cell carcinoma caused by Merkel cell polyana virus. 06:44 It is that that sort of shiny in this case, red colored nodule, which is seen on the tray because of the ear. 06:52 On biopsy the Merkel cell carcinoma at various magnifications and seen with H and E can demonstrate the expected small undifferentiated cells with a very high nuclear cytoplasmic ratio and scanty cytoplasm, as seen on the slides in front of you.
About the Lecture
The lecture BK and JC Virus – Polyomaviruses by Sean Elliott, MD is from the course Viruses.
Included Quiz Questions
Which of the following refers to the shape of the capsid of polyomaviruses?
- Icosahedral
- Dodecahedral
- Prolate
- Helical
- Circular
Reactivation of the BK polyomavirus in an immunosuppressed patient is most likely to involve which of the following organs?
- Kidneys
- Lungs
- Bone
- Brain
- Spleen
Which of the following serotypes of Polyomaviridae is most likely to be associated with the development of progressive multifocal leukoencephalopathy in a patient suffering from acquired immunodeficiency syndrome?
- JC polyomavirus
- BK polyomavirus
- Merkel cell polyomavirus
- KI polyomavirus
- WU polyomavirus
Author of lecture BK and JC Virus – Polyomaviruses

Sean Elliott, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
