Playlist
Show Playlist
Hide Playlist
Biceps Tendonitis, Thoracic Outlet Syndrome and Cervical Radiculopathy


-
Slides Osteopathic Diagnosis of the Shoulder Region.pdf
-
Reference List Osteopathic Manipulative Medicine.pdf
-
Download Lecture Overview
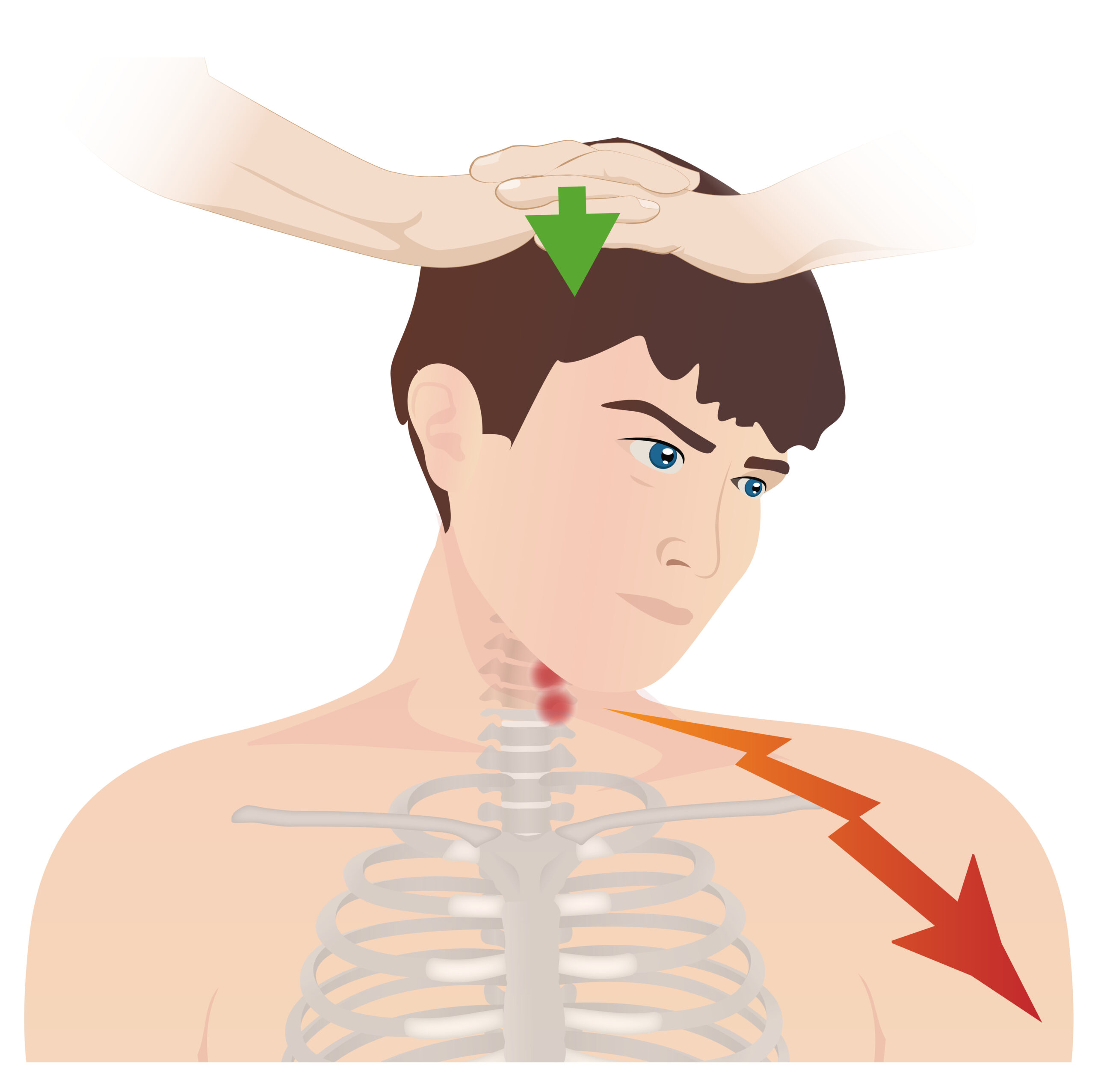
00:01 Bicipital tendonitis is inflammation or degenerative changes at the tendon of the long head of the bicep. 00:07 The long head of bicep runs between the greater and lesser tubercles of the humerus. 00:12 Sometimes due to overuse or repetitive trauma, you could have injury, inflammation in that area. 00:19 There's also a slight slip of a ligament, the transverse humeral ligament, that helps to keep the bicep tendon in place. 00:27 If that ligament is ruptured, that could also cause pain. 00:30 A special test to screen for this is called the Yergason's test. 00:34 Medical management includes rest, ice. 00:37 Sometimes you could have injections in the area for the inflammation. 00:40 You could use nonsteroidals for pain control, or if needed you could use steroid injections to try to decrease some of the inflammation. 00:49 Osteopathic management includes trying to free up the restrictions in the glenohumeral area. 00:55 You want to try to perform myofascial to soften up the area. 01:00 This is a good place that you could perform counterstrain technique to try to decrease any sort of tenderness in the region. 01:06 Yergason's test is a test to evaluate for bicipital tendon instability or tendonitis. 01:12 So remember that the long head of the bicep runs between the greater and lesser tubercles on the humerus with a ligament that covers over the tendon. 01:22 Any sort of repetitive motion, any sort of inflammation, or if that ligament is disrupted, patients complain about anterior shoulder pain. 01:31 So, to perform the test, we start off by having the patient bring their arm to their sides with their elbow flexed to 90 degrees. 01:38 The physician is going to monitor the tendon at the bicipital groove. 01:42 Then we're going to ask the patient to actively externally rotate or supinate their forearm against resistance. 01:49 Remember that the bicep is an elbow flexor and also supinates the arm. 01:54 So, when you ask the patient to supinate the arm, you're activating the muscle. 01:57 If there's any sort of pain in the anterior portion of the shoulder or if the physician actually feels the tendons slipping out of the groove, that is a positive test. 02:09 We could utilize counterstrain for treatment of our patients with bicipital tendonitis. 02:16 There is a point right over the tendon that treats really well with positioning. 02:22 So remember that counterstrain is a passive indirect technique. 02:25 With this technique, what we do is we adjust the joint by putting the patient into a position of comfort. 02:33 So first, we have to identify the point of tenderness. 02:37 Then we will move the joint so that the point is no longer tender. 02:42 That point is also called the mobile point. 02:44 Once we find that mobile point, we hold that position of comfort for 90 seconds at the same time monitoring gently at the region of tenderness. 02:54 After 90 seconds, we should gently bring the joint back to its neutral position and then that point should have decreased pain. 03:03 What we're doing here is we're resetting the muscle spindle of the muscles in the region in order to decrease any sort of spasm and tenderness. 03:12 Thoracic outlet syndrome is a condition where the brachial plexus is being compressed as it exits the cervical spine and travels down the upper extremity. 03:23 Patients will typically complain about a shooting pain going down their arm. 03:28 They may have some numbness and tingling in their hand. 03:31 A special test that we could perform is the Adson's test. 03:34 Usually, what happens is the nerves in the brachial plexus could be compressed in three major spots. 03:40 The first one is between the scalene muscles, the anterior and middle scalenes as the brachial plexus traverses. 03:50 Then comes underneath the clavicle but above the first rib, the costoclavicular space is the second place where the brachial plexus could be compressed. 04:01 Then it could also be compressed behind the pectoral minor near the coracoid process. 04:09 So, there are three major areas where this brachial plexus could potentially be compressed. 04:15 Patients will have neck pain, pain that radiates down the arm. 04:19 Sometimes they'll have diminished pulses in the upper extremities. 04:23 This is because the vasculature runs with the nerves. 04:26 So, if there's compression of the nerves, sometimes there will also be compression of the blood vessels. 04:33 When we treat patients with osteopathic manipulative medicine that may have thoracic outlet syndrome, it's important to remember the anatomy and the course of the brachial plexus and the key areas where they could be compressed. 04:47 So treatment of the scalene muscles is important, treatment of the first rib because the scalene muscles attach to that region. 04:54 If we could relax some of the muscle spasm in the scalene muscles, that could potentially decrease any sort of compression there. 05:00 It's really important to treat the clavicle and the first rib. 05:03 Any restrictions where the clavicle might be depressed or the first rib is elevated, that could also compress the brachial plexus. 05:09 Also looking at the shoulder joint and the regions around the shoulder, any other muscles like the pectoralis minor could also compress on the brachial plexus. 05:21 We also want to treat the cervicothoracic junction and the cervical spine. 05:26 This is because the scalenes attach to the cervical spine. 05:30 You’ll also want to look at different sort of areas that innervate the upper extremities. 05:35 So from C2-T1, there are different nerves that innervate the shoulder and upper extremities, any sort of compression on those nerves can potentially cause those symptoms. 05:44 We also want to free any fascial restrictions located in the thoracic outlet region. 05:49 So, the Adson’s test helps to evaluate for thoracic outlet compression. 05:54 This test is performed by monitoring the radial pulse. 05:58 The neurovascular bundle runs together. 06:02 So, if you have compression of the nerves, at times that might also compress the blood vessels. 06:07 So, what we're doing here is we're checking to see if the vasculature is being compressed and then assuming that that is also occurring for the nerves running with it. 06:17 So, we're monitoring the radial pulse. 06:20 We're going to extend the arm and externally rotate it slightly abducting the arm. 06:24 We're going to ask the patient to rotate and extend their head towards the ipsilateral arm. 06:29 This is going to cause a decrease or absence of the pulse if there's a thoracic outlet compression because you're adding compression to the region in the thoracic outlet with this motion and movement. 06:42 Cervical radiculopathy is impingement of the cervical nerve roots. 06:47 There are many different potential causes. 06:49 Cervical radiculopathy could be caused from a bulging or herniated disc in the cervical spine. 06:54 You could also have narrowing of the region where the nerve roots exit at the foramina. 07:00 Certain degenerative changes could occur that impinges on the nerve roots. 07:05 You could perform a special test to try to recreate the signs and symptoms. 07:10 This test is the Spurling’s test. 07:12 Usually treatment, you start with anti-inflammatories to see if you could decrease the pain. 07:18 However, sometimes surgical management might be required. 07:22 Osteopathic manipulation could be utilized to try to decrease any sort of cervical spine dysfunction. 07:27 Sometimes you could treat the muscle spasms in the cervical region that might be contributing to compression and pain. 07:33 Overall, you could try to improve circulation and lymph flow to help clear the inflammation that's occurring in the region. 07:40 Spurling's test is a special test that could be used to evaluate for cervical nerve root disorder. 07:45 What we're doing is we're narrowing that space where the cervical nerve roots exit. 07:52 So, what we're going to do is we’re going to have the patient gently extend and rotate the patient's head at the cervical spine to the ipsilateral side of the affected shoulder. 08:02 So, if someone is complaining of pain, numbness and tingling, and chilling down their right arm, what you’re going to do is you're going to gently extend, rotate the patient's head towards the right. 08:11 If needed, you could add axial compression. 08:14 If the patient already has pain with just the passive movement, then you should not add the axial compression. 08:20 What you're doing here is you are narrowing that space where the nerve root travels. 08:26 So if there is pain, that is a positive test. 08:29 Here is a list of the special tests that we just reviewed. 08:33 It also has a diagnosis that could be confirmed with the special test. 08:38 Remember that these special tests have different sensitivities and specificities. 08:42 So, just because you have a negative test doesn't always mean that it's not present. 08:47 Just because you have a positive test doesn't mean that they always have that. 08:50 So, you definitely have to take a thorough history, physical examination, and other imaging studies to try to confirm what your patient is presenting with. 08:58 So, in reviewing all these different common shoulder presentations, now hopefully, you have a better understanding of different shoulder diseases, how they present, what tests you could do to try to identify them, and how osteopathic manipulation could be integrated into the identification and treatment of these syndromes.
About the Lecture
The lecture Biceps Tendonitis, Thoracic Outlet Syndrome and Cervical Radiculopathy by Sheldon C. Yao, DO is from the course Osteopathic Diagnosis of the Shoulder Region. It contains the following chapters:
- Biceps Tendonitis
- Yergason`s Test
- Thoracic Outlet Syndrome
- Adson`s Test
- Cervical Radiculopathy
- Spurling`s Test
Included Quiz Questions
Which of the following tests was described in the lecture to be used for evaluating biceps instability or tendinitis?
- Yergason’s test
- Hawkin's test
- Neer test
- Adson’s test
- Ultrasonography test
When performing Adson's test in the evaluation of thoracic outlet compression, which of the following is the position of the patient's head while the physician palpates the radial pulse?
- Rotation and extension toward ipsilateral arm
- Flexion
- Flexion and rotation toward opposite arm
- Extension
- Rotation toward opposite arm
While the physician is monitoring the biceps tendon, what is the patient instructed to do during a Yergason’s test?
- Supinate the forearm against resistance
- Flex the wrist
- Resist all motion
- Assist all motion
Which of the following tests may be used in the detection of impingement of cervical nerve roots?
- Spurling’s test
- Neer test
- Adson’s test
- Ultrasonography
- Yergason’s test
Author of lecture Biceps Tendonitis, Thoracic Outlet Syndrome and Cervical Radiculopathy

Sheldon C. Yao, DO
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
