Playlist
Show Playlist
Hide Playlist
Axillary and Long Thoracic Nerves – Nerve Lesion of Upper Limb

-
Slides 10 UpperLimbAnatomy Pickering.pdf
-
Download Lecture Overview
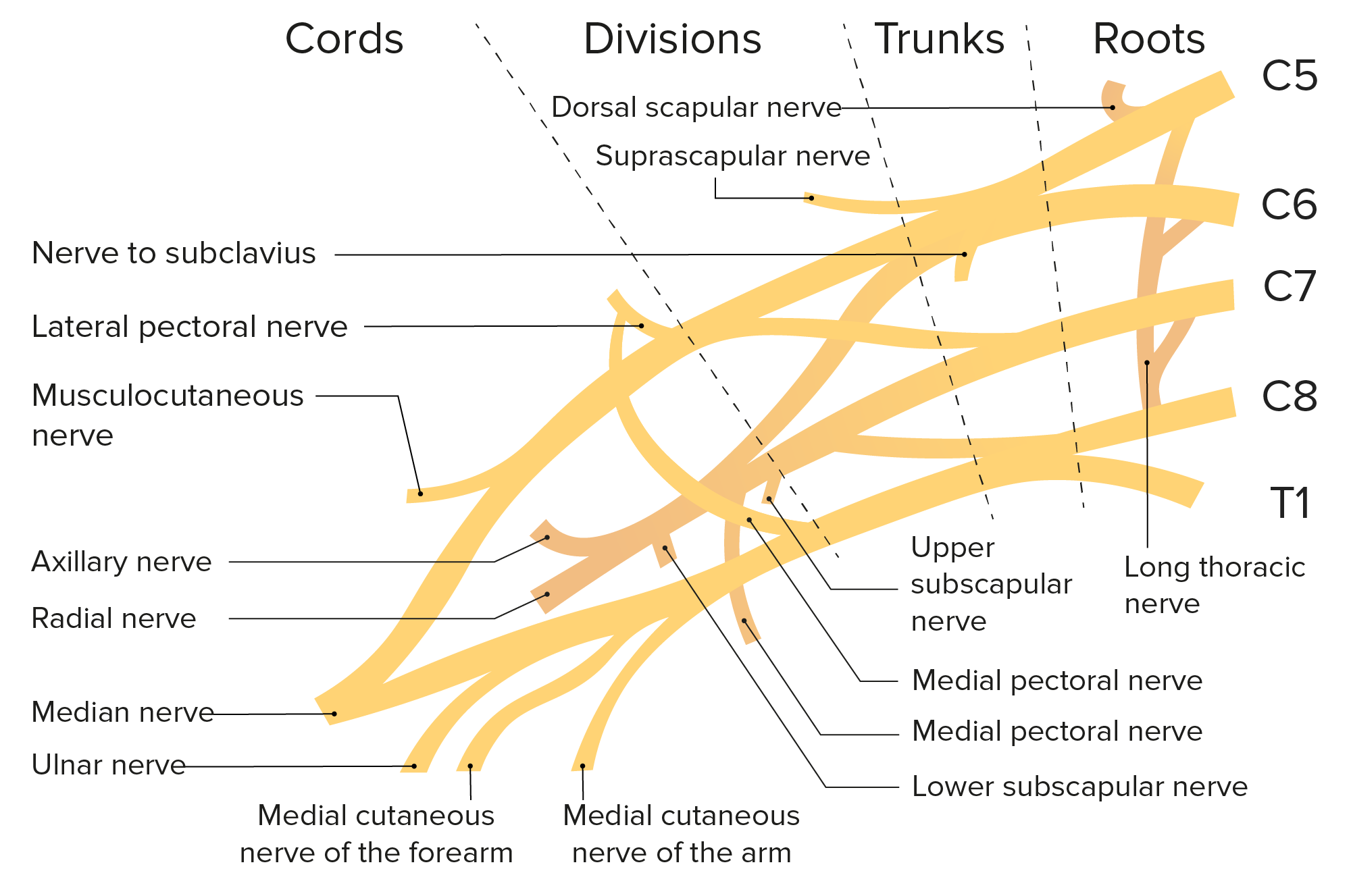
00:00 So let’s have a look at the axillary nerve. 00:03 Remember the axillary nerve passing through the quadrangular space, we can see it here, passing through the quadrangular space with the posterior circumflex humeral artery to go and supply deltoid. We can see this on the posterior view of a right shoulder. 00:19 So damage to the axillary nerve could occur as a fracture to the surgical neck of the humerus, also due to compression of the muscles that form the quadrangular space. So, if the muscles that form the quadrangular space were to become bigger, that’s a hypertrophy, then this could compress the quadrangular space. Now as we know passing through the quadrangular space as I just said is the axillary nerve, then this can compress this nerve leading to functional deficits of the deltoid. If there’s a fracture to the surgical neck of the humerus, then as the axillary nerve passes through here, then the same problems will result. You’ll have paralysis of the deltoid muscle. 00:59 Paralysis leads to atrophy of the muscle, and this can lead to loss of the rounded shoulder contour as you lose the muscle mass. Now, deltoid is involved in abducting the arm, but it abducts it after the first 15 degrees. So the first part of abduction is carried out by supraspinatus, and that starts the abduction as the first 15 degrees, and then the deltoid muscle carries on. So the individual will only be able to abduct their arm due to supraspinatus by 15 degrees. You’d also have sensory loss over a patch of skin on the lateral arm which we can see here. This little patch of skin over the lateral aspect of the arm, shoulder region, is due to the cutaneous branches coming from the axillary nerve. And here, we can see that they would be damaged. So you’d have loss of sensory distribution from this region. If we then look at the long thoracic nerve, the long thoracic nerve comes away from the brachial plexus and it runs down, we can pick up the long thoracic nerve here. It’s running alongside serratus anterior, and it actually runs superficial to serratus anterior. Here, we’re looking at the right side of the thoracic cavity. This is anterior, this is posterior, this would be deltoid here. 02:22 And we can just see the long thoracic nerve running down here to supply serratus anterior. 02:27 So damage to the long thoracic nerve that’s coming from the brachial plexus can be due to damage to the lateral thoracic wall. This can be due to a fight or it could be due to surgery on the lateral aspect of the chest wall. If there’s surgery on the breast or if there’s removal of lymph nodes in this region, then the long thoracic nerve could be damaged. The effect is that the medial border of the scapula would protrude through the skin, especially when the patient is asked to push against the fixed wall, and this is known as winged scapula. So serratus anterior is important in clamping the scapula onto the posterior chest wall. It holds the scapula onto the chest wall. 03:11 So damage to the long thoracic nerve would paralyze this muscle, and therefore, when you’d go to move your arm and you need your scapula to be anchored to make it a stable push off, then that’s not going to be possible, and the scapula is then pushed into the skin, and that gives the impression of a winged scapula. The actual triangular shape of the scapula is seen as an impression on the under surface of the skin.
About the Lecture
The lecture Axillary and Long Thoracic Nerves – Nerve Lesion of Upper Limb by James Pickering, PhD is from the course Upper Limb Anatomy [Archive].
Included Quiz Questions
Which fingers lose cutaneous sensation when the median nerve is damaged?
- Lateral three-and-a-half
- Lateral four-and-a-half
- Lateral 4
- Lateral 3
- Lateral two-and-a-half
Which muscle is paralyzed when the long thoracic nerve is injured?
- Serratus anterior
- Pectoralis major
- Pectoralis minor
- Deltoid
- Trapezius
Which statement regarding injury to the axillary nerve is correct?
- It can cause paralysis of the deltoid muscle.
- It can cause loss of the first 15 degrees of abduction.
- It can cause paralysis of the trapezius muscle.
- The teres minor will be spared.
- It will cause winging of the scapula.
Author of lecture Axillary and Long Thoracic Nerves – Nerve Lesion of Upper Limb

James Pickering, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
simple and sorted. well explained and very good concept builder
