Playlist
Show Playlist
Hide Playlist
Autonomic Nervous System


-
Slides OMM Pulmonary System.pdf
-
Reference List Osteopathic Manipulative Medicine.pdf
-
Download Lecture Overview
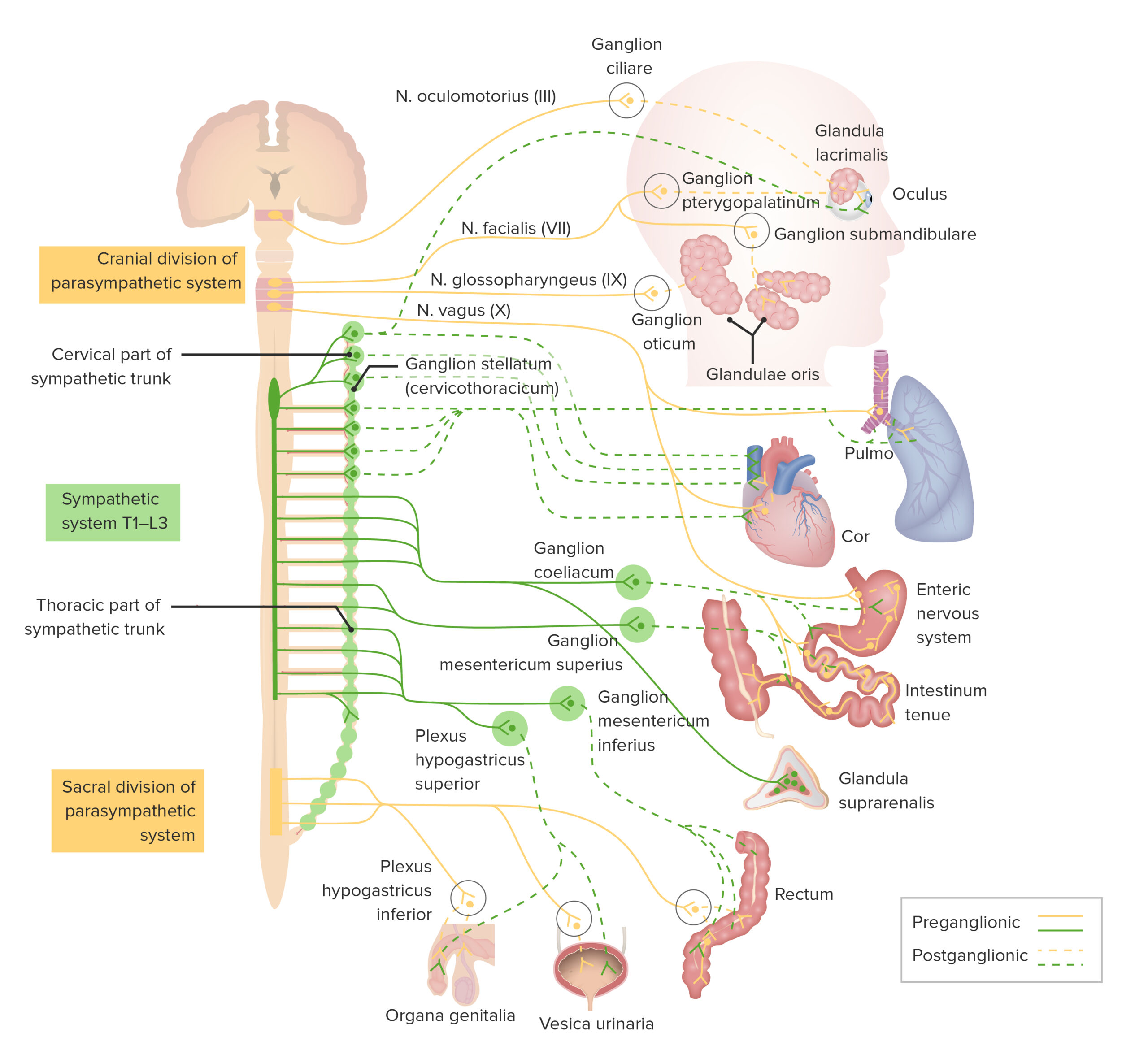
00:01 The other concept to pay attention to is the autonomic nervous system and the sympathetic and parasympathetic, because these are going to affect breathing and can help or hurt breathing. 00:13 When you think about the sympathetics, those are thoracic segments. 00:16 T1 through T5, they innervate the lungs. 00:20 They're going to cause bronchodilatio,n and they're going to affect the mucous secretions, both the amount and the thickness. 00:26 So you want to make sure you have optimal viscosity so that it can bay the lungs and enhance oxygen exchange, but not block oxygen exchange. 00:35 The autonomic nervous system is critical for monitoring what's going on with breathing. 00:41 You have nociceptors which tell you about the pressure and what's happening within the lungs, and they feed back into the autonomic nervous system through the upper thoracic communication pathways. 00:54 And again, a lot of the information is coming from the upper thoracic region. 00:58 The vagus nerve is what's going to moderate, moderate, the parasympathetic innervation of the lungs. And that's what's going to cause bronchoconstriction and increase mucous production in the lungs. 01:11 And the nociceptors from the smaller airways which go through the vagus are going to moderate what's going on in asthma and small airway disease and let the body know what needs to be done. The vagus has been shown to reflex with the upper, upper cervical spine and that pathway is through C two and the sensory ganglion of the vagus are found at the OA and jugular foramen. When you treat segmental dysfunction, it's important to focus on those areas because that will enhance physiologic function and prevent a spiraling down and deterioration in the area. 01:47 The other goal is to decrease the use of inhalers and most studies of OMM and pulmonary disease use that as a secondary endpoint, which is hospitalizations and the medications used. 01:59 Lymphatics also need to be taken into consideration as a secondary system for bathing the lung and returning fluids to the lung. 02:09 And in asthma and pneumonia. 02:11 You may want to check the lymphatic return and understand what's going on with the pulmonary lymphatics, both in the chest wall cavity and making sure that you address that issue as well because pulmonary lymphatics dump into the vasculature but have their own system for distribution. 02:28 The airways are drained by the lymphatics, but they also have blood supply as well. 02:33 And this is moderated by mucociliary mechanisms. 02:38 The mucociliary mechanisms doesn't extend to the terminal bronchioles of the or the alveoli. So the drainage is going to be a separate system and discrete. 02:48 Paying attention to pulmonary lymphatics, particularly in asthma and pneumonia. 02:52 We'll help you understand what needs to be, what needs to be treated and how drainage is occurring through the lymphatics. 02:59 So the pulmonary lymph is enhanced with respiration, with excursion. 03:04 You're going to have return of the lymph and dumping of the lymph into the vascular system. So pay attention to the respiratory excursion and make sure that adequate return is being allowed. 03:15 When you treat the pulmonary patient, make sure you pay attention to positions of comfort, examine them for paradoxical versus fluid motion. Do what you can to improve the efficiency of the respiratory musculature so that they can breathe comfortably, reduce segmental facilitation as a way of allowing communication to occur and the body to heal itself and do what you can to improve lymphatic drainage. 03:40 I pay a lot of attention to the ribs, making sure that you do have good pump handle and bucket handle motion and secondarily to the vertebrae where the ribs attach because that's going to eventually become a problem as well. 03:54 So that's my talk on the respiratory effects, on the musculoskeletal system, and the role of OMM and pulmonary conditions. 04:03 Thank you.
About the Lecture
The lecture Autonomic Nervous System by Tyler Cymet, DO, FACOFP is from the course Osteopathic Treatment and Clinical Application by System. It contains the following chapters:
- Autonomic Nervous System
- Pulmonary Lymphatics
Included Quiz Questions
The sympathetic innervation of the lungs causes bronchodilation and originates from what thoracic segments?
- T1–T6
- T5-T9
- T10–T12
- T10–L2
Which of the following are OMM treatment goals when treating patients with pulmonary conditions? (Select all that apply)
- Improve compliance and excursion of the thorax.
- Improve the efficiency of respiratory muscles.
- Improve lymphatic drainage.
- Reduce segmental facilitation.
- Increase respiratory rate and drive.
Author of lecture Autonomic Nervous System

Tyler Cymet, DO, FACOFP
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
