Playlist
Show Playlist
Hide Playlist
Auscultation of the Heart: Heart Sounds


-
Reference List Physical Examination.pdf
-
Download Lecture Overview
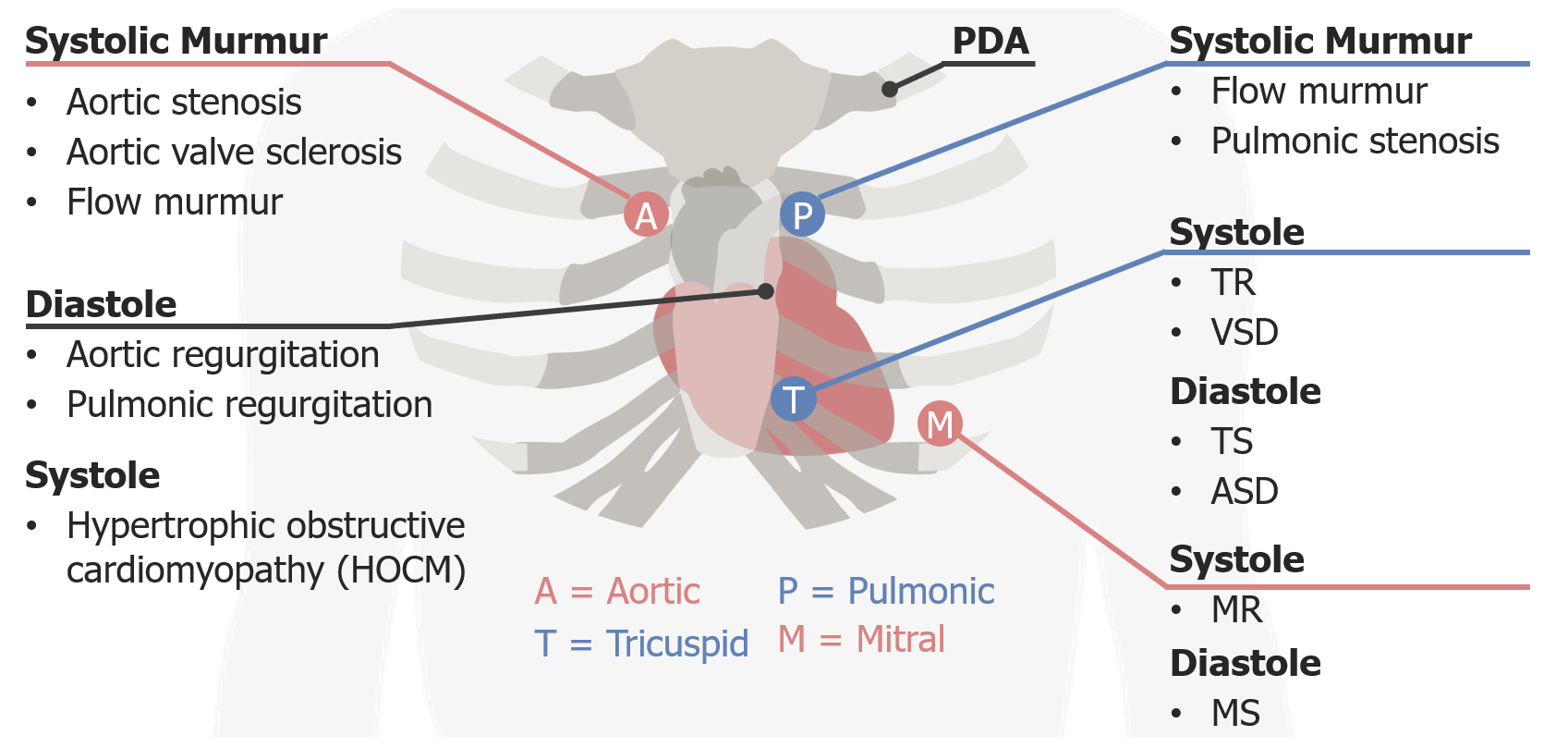
00:01 With that, let's talk about the cardiovascular exam. 00:04 So, when you know the cardiac exam, many things are possible. 00:10 Now, what do I mean by that? Many things are possible is actually not just a statement of fact, it's also an acronym, it's a useful way to remember the heart valves. 00:20 Many things are possible is MTAP, let me just draw that here, M-T-A-P. 00:35 Those letters represent the sequence of closing of the four heart valves in the heart, mitral, the tricuspid, the aortic, and the pulmonic; and using that acronym, many things are possible, you'll remember which sequence those valves are closing, you'll also remember where they're located. 00:54 This is a circle M-T-A-P-M-T-A-P, which helps us to keep track of where we are when we're listening for particular murmurs and trying to find the etiology of a particular murmur that we hear based on the location on the anterior chest wall. 01:10 The next thing we talk about is once we lay our stethoscope on his chest, we're going to be listening in particular to three phases of the cardiac cycle. 01:20 You're going to listen first to heart sounds, that's is your S1 and S2, also known as your lub-dub, lub-dub, lub-dub. 01:27 We're going to listen to the S3 and S4 parts of the heart sounds as your gallops which can accompany your lub-dub and lub-dub. 01:34 The second part is systole, so we're going to focus very deliberately on listening on the space between S1 and S2; and then we're going to listen to diastole, the space between S2 and S1, and I found it really important when you're auscultating the chest, to make sure you really very deliberately listen to one thing at a time, first the heart sounds, then systole, then diastole. 01:59 That helps you avoid the common mistake of getting so sucked into a very loud systolic murmur that you neglect to hear that more subtle diastolic murmur that's happening afterwards. 02:10 Alright, so with that opening outline, heart sounds, systole, diastole, let's start off by talking about the heart sounds. 02:17 So S1 and S2, lub-dub, lub-dub. As we said before, many things are possible so M and T are the first heart sounds so that must represent S1, and then AP represent the second heart sound, S2. 02:34 These are paired together because they're so closely occurring in space all we hear is a lub not two different sounds just the lub, and then the dub, is the A and the P. 02:43 Now, normally, when you are simply breathing, just comfortable tidal volume breathing, the mitral and tricuspid valves are closing almost perfectly synchronously. 02:56 However, the aortic and the pulmonic valve will actually separate or split during the respiratory cycle specifically during inspiration. 03:07 So what happens is if this S1 here, mitral and tricuspid; and this is your S2, aortic and pulmonic, when the person takes a deep breath, the aortic and the pulmonic will actually separate like so, [breathing], and that's normal physiology and that's driven by the fact that when you take a deep breath, you're creating a negative space in his chest that's actually drawing more blood to the right side of the heart. 03:42 If there's more blood in the right side of the heart, its going to take longer for that pulmonic valve to close, and so the pulmonic valve moves farther away in time while the aortic valve stays largely in the same place. 03:56 That's called physiologic splitting, we expect to hear that. 03:59 When you're listening to the chest in this area, you should listen to make sure that when he's inspiring, when he's inhaling, those -- that second heart sound does split like that. 04:09 In contrast, there are some instances where for example, the aortic valve may actually be displaced in time, particularly with the left bundle branch block. 04:20 Now, if you have a left bundle branch block, the left ventricle is going to contract later than it's supposed to, so rather than having your S1 here and your S2 here, with aortic and pulmonic valve, these two are actually flipped like so -- the aortic valve is now over here and the pulmonic valve is here, so when this person takes a deep breath, the pulmonic valve moves over [breathing]. So when you're hearing is paradoxic, you're hearing during inspiration with two heart sounds moving closer together, next, because the pulmonic valve is moving away where it supposed to but the aortic valve is so delayed by the bundle branch block that you hear the pulmonic valve catching up with it during inhalation. 05:10 So that's called paradoxic splitting, that you'll see with left bundle branch block and a few other conditions. 05:16 We're not going to into all the details of the different things that can cause abnormal splitting, but I just wanted to highlight that that's an important thing you can pick up on by just listening very closely to those heart sounds. 05:27 Importantly, the S1 and S2 heart sounds are higher in pitch than some other sounds that you might hear, and this leads me to our important quick brief on your stethoscope. 05:39 Your stethoscope has two heads on it, you've got a bell, you've got a diaphragm. 05:44 These are useful in different circumstances. 05:47 In particular, the bell of your stethoscope is most useful for low pitch sounds. 05:52 It actually by putting the bell on the chest and creating a seal, you are filtering out a lot of the higher pitch sounds. 05:58 In contrast, the diaphragm is useful for hearing all of the different pitches within the heart thought with potentially a little bit of a focus on some of the higher pitch sound. 06:08 So when you're using the diaphragm, you're thinking higher pitch; the bell, you're thinking lower pitch. 06:13 So I just said that the S1 and S2 heart sounds, we know that there are -- we're going to best hear S2 up here, we're going to best hear S1 down here, and typically, you're listening with the diaphragm cuz they're both higher pitch sounds, like so. 06:54 Now, in some patients, you may find that rather than just hearing the simple lub-dub, lub-dub, lub-dub, maybe you'll hear an extra sound, something like a, ba-lub-dub, ba-lub-dub, ba-lub-dub. 07:09 That is an extra heart sound, in this case a ba, occurring before the lub, and that's called an S4, it immediately precedes systole and it's called a fourth heart sound, it's part of the atrial kick. 07:23 What's happening when you hear an S4 is that the left ventricle has fully, fully-filled during diastole, you had diastolic filling, and that end of that diastole, the left atrium is contracting and spitting out that last volume of blood from the atrium, but its hitting against the stiff left ventricular wall, and this is something that you'll hear in patients with left ventricular hypertrophy, potentially hypertrophic obstructive cardiomyopathy, and it's a very characteristic feature that you'll find in a lot of folks and it does portend or suggest that a patient does have one of those conditions. 08:01 Importantly, that the ba-lub-dub, the ba, is a lower pitch sound. 08:06 As I said before, that means you're going to best catch it with the bell of your stethoscope. 08:11 Before we find it though, let's just quickly talk about the other kind of abnormal gallop that you might hear. 08:17 Rather than lub-dub, lub-dub, lub-dub, you might hear a labdibub, labdibub, labdibub, labdibub. 08:26 Essentially, that is a sound happening right after S2 so rather than lub-dub, its labdibub, labdibub, and you can tell that bub is coming right after the du, which would have been a dub, and that is an indication of an S3, a third heart sound. 08:46 Now, our third heart sound is also emanating from the left ventricle down here at the apex of the heart, and rather than being associated with left-ventricular hypertrophy, it's typically found in a acute systolic heart failure with left ventricular dilation, potentially increased filling pressures, and almost always, some evidence of systolic heart failure, whether it's in the setting of ischemic cardiomyopathy, or potentially, if somebody has aortic regurgitation with a surplus of blood back filling into the heart then has to be ejected. 09:17 So that sound is also heard at the apex, which is where, of course, the left ventricle is going to be best heard, and it's also a low pitch sound, just like the S4. 09:26 So the ideal way to bring about that sound, it's going to be with the bell and since we really want to try and accentuate that sound cuz it can be very subtle to hear, or I should going to reposition our patient and lie him in the left lateral decubitus position to really bring out that heart sound. 09:44 With that, let's take a listen to the apex of the heart. 09:50 Alright, so now that we have Shawn in the left lateral decubitus position, this is the ideal place for us to try and pick up a third or fourth heart sound. 10:02 I've got the bell of my stethoscope lightly applied to his chest simply to provide a seal. 10:07 If I push too hard, I'm actually just creating a diaphragm out of the skin so you just want to have light pressure at the apex, and that's it. 10:23 Now, there's a couple of different positions that you may see over the course of this next few minutes depending upon what you're looking for. 10:31 You may have him lying in the left lateral decubitus position, you may have him sitting upright, you may have him laying flat. 10:37 In general, you don't want to have to repeat the entire cardiac exam in all three positions, so as we go through each murmur, each type of valvular disease, I'll talk about which positions maybe most appropriate.
About the Lecture
The lecture Auscultation of the Heart: Heart Sounds by Stephen Holt, MD, MS is from the course Examination of Cardiovascular and Respiratory System.
Included Quiz Questions
What cardiac physiology does the S1 heart sound represent?
- Closure of the mitral and tricuspid valves
- Closure of the aortic and pulmonic valves
- Increased ventricular filling pressures, such as in heart failure
- Atrial contraction against a stiff ventricle, as seen in left ventricular hypertrophy
- Ventricular contraction
What cardiac physiology does the S2 heart sound represent?
- Closure of the aortic valve and pulmonic valves
- Closure of the mitral and tricuspid valves
- Increased ventricular filling pressures, such as in heart failure
- Ventricular contraction
- Atrial contraction against a stiff ventricle, as seen in left ventricular hypertrophy
What cardiac physiology does the S3 heart sound represent?
- Increased ventricular filling pressures, such as in heart failure
- Closure of the aortic valve and pulmonic valves
- Closure of the mitral and tricuspid valves
- Ventricular contraction
- Atrial contraction against a stiff ventricle, as seen in left ventricular hypertrophy
What cardiac physiology does the S4 heart sound represent?
- Atrial contraction against a stiff ventricle, as seen in left ventricular hypertrophy
- Closure of the aortic valve and pulmonic valves
- Closure of the mitral and tricuspid valves
- Ventricular contraction
- Increased ventricular filling pressures, such as in heart failure
What is TRUE regarding physiologic splitting of the second heart sound (S2)?
- The splitting gets more pronounced with inspiration, as it takes longer for the pulmonic valve to close.
- The splitting gets more pronounced with inspiration, as it takes longer for the aortic valve to close.
- The splitting gets more pronounced with inspiration, as it takes longer for the mitral valve to close.
- It is an abnormal finding when splitting gets more pronounced with inspiration.
- Physiologic splitting is not heard in a patient with a left bundle branch block.
Author of lecture Auscultation of the Heart: Heart Sounds

Stephen Holt, MD, MS
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
10000000 x better than "medical school." I think medical school actually makes you dumber. This is the way to go.
Los videos están muy claros y son muy útiles, muchas gracias!
Very comprehensive and detailed explanation of cardiac cycle and sounds.Thank you.
perfect explanation for good foundation of the cardiovascular physical examination
1 customer review without text
1 user review without text
