Playlist
Show Playlist
Hide Playlist
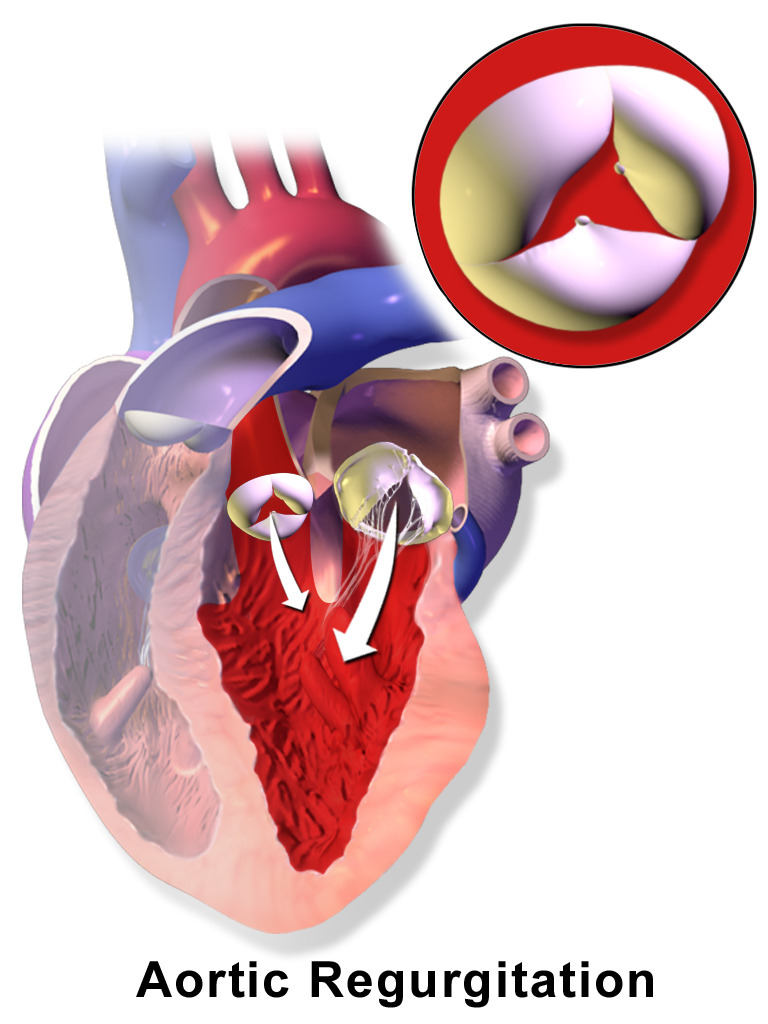
Aortic Regurgitation: Pathogenesis

-
Slides Valvular Heart Disease Aortic Regurgitation Cardiovascular Pathology.pdf
-
Download Lecture Overview
00:00 Let us take a look. Aortic regurg. Abnormality of backward flow. 00:06 When is your aortic valve supposed to close? Are you having problems with closing or opening? Aortic stenosis, close your eyes, was it difficult to it, aortic valve, opening right. That was a systolic type of murmur whereas with aortic regurg you have a problem with the aortic valve closing. Which way does it close? Here my aorta, here is my left ventricle, it is supposed to close this way but it is not. It does not want to close so therefore, there is going to be regurg. 00:37 When is it supposed to close? During diastole. So what kind of murmur is aortic regurg? A diastolic murmur. Your next question is well, is it early or mid? I will show you a picture where you will clearly see why it is an early diastolic murmur. 00:53 Results from valve leaflets issues, aortic root such as congestive heart failure or marfan, what happens in marfan. It is the fibrilin type of issue you are referring to chromosome 15 FFF, our elastic tissue is not being formed properly and so, therefore, there might be widening of the aortic root, welcome to aortic regurg, congestive heart failure, Ehlers-Danlos, widening of the aortic root. Could it be some type of infection? Well what if you had a patient who was in the armed forces and was away from home for a long period of time and this patient had urges and didn’t exactly use proper judgment and comes back with issues with aortic regurg. You have heard of syphilitic aortitis haven’t you? Syphilitic aortitis, what happens? There is something called arteritis obliterans. You have talked about all these in microbiology. Just put it together here and please understand that the number of differentials that you have with aortic regurg. Causes, talked about this with aortic stenosis. 02:05 Dr. Raj, why is rheumatic heart disease here with aortic regurg? Do you remember me telling you first and foremost developing ,countries is what you are looking at with rheumatic heart disease, number 1. Number 2, we talked about the organism being something like streptococci pyogenes, Group A streptococci also referred to something like pharyngitis in which the patient, the child, perhaps wasn’t properly, inadequately treated resulting in two to four weeks later issues with the heart. We talked about all that. Next, Early on you are going to cause damage to the valve. You tell me, what valves predominantly are going to be affected in rheumatic heart disease? Left side, 95 percent of the time and so you pay attention to that. Is that clear? On the left side, early on what kind of damage is it? It is regurg, it gets floppy, vegetations. At some point, you begin the repair process. What does repair meant to you? Talk about fibrosis. Some may result in stenosis and hence in aortic stenosis we also had rheumatic heart disease but it's a chronic type. Developing countries. And in developed countries, what are you looking at? Interesting now, we'll slow down here, look at me, pay attention. If it is a bicuspid aortic valve first off you know it's a young patient. The fact that you even have bicuspid is a congenital issue, the last time we talked about this was in a previous discussion of aortic stenosis when we said that by having bicuspid that you might have damaged tissue resulting in dystrophic calcification and what does that result in? That was aortic stenosis, absolutely correct. So, in developed countries, in which a patient who is young may result in aortic regurg at some point, aortic stenosis bicuspid may also result in regurg, is that clear? And do not miss this question. This is where students tend to get confused because they are so black and white. You know certain things you absolutely have to keep separate but at the same time understand the continuum. You don’t want to be so black and white that you miss a question because "Oh, it has to be this." No, it doesn’t have to be anything. The process is important, so even bicuspid congenital aortic valve may have aortic stenosis, what kind of murmur was that? A crescendo-decrescendo. A systolic murmur, or it could be a diastolic murmur. Where would you hear this early diastolic murmur, please? Left parasternal moving towards apex, maybe perhaps your third intercostal space. I hope that's clear. You spend little bit of time with this paragraph. Let's move on. 04:57 What else may happen? It might cause damage due to infectious endocarditis, marfan syndrome, trauma maybe perhaps even aortic dissection. With aortic dissection, imagine what may happen? You might have stabbing back pain and when you have stabbing back pain, if you have enough dissection is it possible that you might then have retrograde flow through the aortic root and cause widening and expansion of the aortic root? Of course and so your aortic regurg may be present and may be even perhaps the blood is rushing in a very rapid manner into the pericardial cavity. 05:32 What is that called, rushing rapidly? Tamponade. A lot of things we are putting together because it is not just bullet points in which you are memorising. You are bringing in information in which you are setting the foundation and building. Aortic regurg has developed, then you have more blood coming in, what is the ventricle going to do? It will then cause increased size hypertrophy resulting in what is known as eccentric hypertrophy. Just like we have
About the Lecture
The lecture Aortic Regurgitation: Pathogenesis by Carlo Raj, MD is from the course Valvular Heart Disease: Basic Principles with Carlo Raj.
Included Quiz Questions
Which of the following is true regarding aortic regurgitation?
- The aortic valve is unable to close.
- The aortic valve is stiff and has difficulty opening.
- There is a systolic murmur.
- No murmur is heard until later in older adulthood.
- The most common cause in developed countries is rheumatic heart disease.
Which of the following is an unlikely cause of aortic regurgitation?
- Congenital rubella infection
- Rheumatic heart disease
- Congenital bicuspid aortic valve
- Aortic dissection
- Marfan syndrome
Which of the following best describes the murmur in aortic regurgitation?
- Early diastolic murmur
- Late diastolic murmur
- Crescendo-decrescendo systolic murmur
- Holosystolic murmur
- Early systolic murmur
Author of lecture Aortic Regurgitation: Pathogenesis

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
