Playlist
Show Playlist
Hide Playlist
Anomalies of the Aging Brain: Parkinson's Disease

-
Slides 03 AnomaliesAgingBrainParkinsonHuntington Aging.pdf
-
Download Lecture Overview
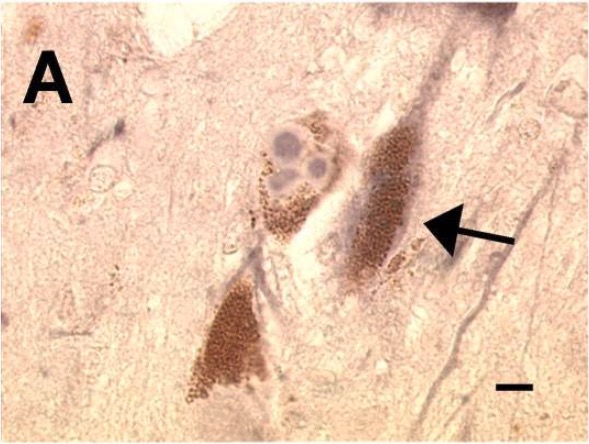
00:01 In this lecture, we’ll take a look into Parkinson’s and Huntington’s disease and discuss all of the things that you need to know about both of those. Beginning with Parkinson’s disease, it is a little bit different than Alzheimer’s because this is a disease that affects movement first rather than memory. 00:24 So, it is a progressive neurodegenerative disorder. It involves damage to dopaminergic neurons in the basal ganglia. We’ll take a look more closely at that shortly. You’re probably familiar with this fairly standard presentation of Parkinson’s. We see the tremors with a little bit of shakiness and stiffness, slowed movements that appear to be sort of difficult to start. Balance issues also arise. 00:56 Now, the basal ganglia, to give us some orientation are a number of nuclei in the subcortical area of the brain. The ones that we’re particularly interested in are the substantia nigra and the striatum. 01:14 It turns out that there’s communication between these two regions of the brain that gets broken down in Parkinsonism. So, let’s take a little bit closer look at the two pathways involved in controlling movements. First of all, we have a direct pathway in which the substantia nigra has dopaminergic neurons that signal the striatum. Dopamine is deposited in the striatum. 01:40 Then that message is then passed on through the thalamus into the cortical regions of the brain that are appropriate for the desired movements. Now, this is an excitatory pathway where we’re acting to increase the level of movement. So, I like to use the thalamus as an example of an analogy here, a puppy or a little dog that lives in the thalamus. He’s very excited and stimulated through this substantia nigra striatum pathway with dopamine. So dopamine makes the dog pretty happy. 02:16 He could run all over the cortex but that’s not going to go so well. So, we have also an indirect pathway that works through a number of other neurons, nuclei in the basal ganglia. That acts more like a leash holding the dog in the realm that it should be. So, we have a direct pathway that acts to increase movements and an indirect pathway that acts to decrease or fine tune the movements. 02:51 That is the leash. When we consider Parkinson’s, we’re looking at this direct pathway and having a problem with increasing the movements. So that’s where we see the symptoms of Parkinson’s, it being difficult to initiate movement because this nigrostriatal pathway is shut down. 03:17 It is shut down due to an accumulation of Lewy bodies. Where have you heard me mention Lewy bodies before or maybe you haven’t. But if you have, it was in another lecture where we were considering Alzheimer’s and different sorts of dementia, not only Alzheimer’s but there was a Lewy body dementia. Now, I’m going to speak a little bit more about these Lewy bodies because there’s something that you need to understand. First of all, understand that we don’t really know quite how they function but I’ll let you know what we do know. 03:57 First of all, we do know that these Lewy bodies involve a protein called α-synuclein and accumulation of it, so again, clamping of a protein that interferes in signaling. 04:11 Thus, a neuron that’s no longer sending signals tends to degenerate and eventually will result in neuronal death. We can see these clusters of proteins interfering with mechanisms of the cell. 04:25 When 80% of the neurons at the nigrostriatal pathway have degenerated, signals have become low enough or slow enough that we start seeing this bradykinesia. Bradykinesia is that slowed, hard initiation of movement patterns. It tends to look fairly rigid so movements are no longer smooth and coordinated. They’re a little bit jerky. That’s where we may see the tremors. 05:03 The sad thing is with Parkinson’s, we also see spreading to other regions of the brain where we start seeing progression into dementia later on in the disease. So Lewy bodies, we know some about. The question is though, are they a cause of or a result of Parkinson’s disease? It turns out that we are not really too certain about that. The cause of Parkinson’s is still fairly much of a mystery. Most cases seem to be idiopathic which really means we don’t know. 05:49 They appear to arise spontaneously. Fifteen percent or so of cases do have a genetic link. 05:57 We know that there are some serious environmental factors that are associated with Parkinson’s disease. The first and I think the most controllable that we have are these pesticide exposures or other chemical exposures. There’s a high correlation between people that are working in farm and the farming industry where pesticides are applied heavily to crops having a very high incidence of Parkinson’s disease. Also individuals that experience a lot of cleaning chemicals and have inhalation of heavy metals, so all these chemicals affecting the neurons and generation of these Lewy bodies. Also, you’ve probably heard quite a bit about having history of concussions leading to some dementias as well as Parkinson’s disease. 06:55 So, those are certainly risk factors also. With Parkinson’s, it seems to show up more frequently in males than it does females. So, we have increased gender risk in the case of Parkinson’s disease.
About the Lecture
The lecture Anomalies of the Aging Brain: Parkinson's Disease by Georgina Cornwall, PhD is from the course Aging.
Included Quiz Questions
Which of the following statements regarding the onset of Parkinson's disease is true?
- The pathology starts in the basal ganglia
- The pathology starts in the temporal lobe
- The disease presents with memory problems first, then movement disorder.
- The disease pathology begins in the indirect movement pathway.
- The disease has not yet been associated with harsh environmental chemicals, such as pesticides and cleaning fluids.
Which of the following is true regarding the pathophysiology of Parkinson's disease?
- Lewy bodies accumulate in the nigrostriatal pathway, interrupting excitatory dopaminergic neuronal signaling in the direct movement pathway.
- Lewy bodies accumulate in the nigrostriatal pathway, interrupting inhibitory dopaminergic neuronal signaling in the direct movement pathway.
- Lewy bodies accumulate in the nigrostriatal pathway, interrupting excitatory dopaminergic neuronal signaling in the indirect movement pathway.
- Lewy bodies accumulate in the nigrostriatal pathway, interrupting inhibitory dopaminergic neuronal signaling in the indirect movement pathway.
- Lewy bodies are alpha-synuclein protein clumps seen in Lewy Body dementia only.
Which of the following symptoms is typically not seen until the end-stage of Parkinson's disease progression?
- Dementia
- Bradykinesia
- Rigidity
- Difficulty initiating movement
- Difficulty with balance
Which of the following has NOT been linked to the development of Parkinson's disease?
- History of cardiovascular disease
- Heavy metal inhalation and harsh chemical exposure
- History of multiple concussions
- Male gender
- Genetics
Author of lecture Anomalies of the Aging Brain: Parkinson's Disease

Georgina Cornwall, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
3 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Very clear and thorough, liked it a lot thank you Dr Cornwall!
2 customer reviews without text
2 user review without text
