Playlist
Show Playlist
Hide Playlist
Allergic Bronchopulmonary Aspergillosis (ABPA)

-
Slides Pulmonary diseases in older children.pdf
-
Download Lecture Overview
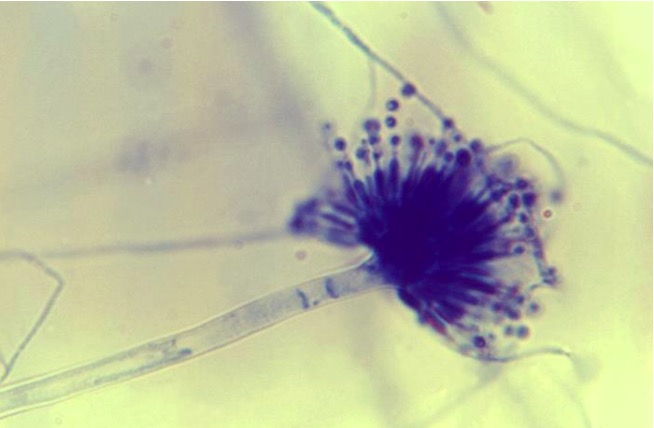
00:01 Let’s switch away from pulmonary embolism and talk about allergic bronchopulmonary aspergillosis or ABPA. 00:10 This is something we see in children not that infrequently and we should all be aware of it. 00:16 So ABPA is a hypersensitivity to Aspergillus, which is in the environment almost ubiquitously. 00:25 Maybe you haven’t seen before, it’s only present in 1% to 2% of patients with asthma, and a higher percentage, 7% to 9%, of patients with cystic fibrosis. 00:38 This is an antibody mediated through IgG and IgE response to Aspergillus that’s getting in the airway. 00:47 If you will, the Aspergillus gets in and then there’s a hyperresponsiveness to that Aspergillus, sort of like a type 1 autoimmune response, where there’s more antibodies going in and attacking the Aspergillus inappropriately. 01:05 This in turn results in inflammation, bronchial obstruction, mucus production. 01:12 These patients are at risk for eosinophilic pneumonia and you may see even granulomas on chest x-ray. 01:19 When do we think about allergic bronchopulmonary aspergillosis or ABPA? We typically think about it in a child with asthma or cystic fibrosis, who isn’t responding to standard therapy for their respiratory condition. 01:34 We can get a skin prick and notice increased sensitivity to Aspergillus, a wheal will be raised where the Aspergillus protein was injected into the skin, or we can check titers in the blood for IgE and notice a very high IgE level, which is consistent with the disease. 01:56 Patients on chest x-ray will show infiltrates that are not responding to standard antibiotics. 02:02 And what’s interesting here is that a CBC may in fact be helpful because you may see eosinophilia on the CBC, which is not really looking for a high white count, but particularly looking for high levels of eosinophils. 02:17 If a patient has ABPA, we will typically treat them with itraconazole, which is targeted against the Aspergillus, which is causing the systemic symptoms. 02:28 We will often put these patients on steroids and it’ll be a prolonged steroid taper over three to six months to avoid relapse. 02:38 So these patients often have problems with their steroids. 02:43 We’re going to monitor their IgE levels and follow their chest x-ray for resolution of symptoms.
About the Lecture
The lecture Allergic Bronchopulmonary Aspergillosis (ABPA) by Brian Alverson, MD is from the course Pediatric Pulmonology.
Included Quiz Questions
Which of the following drugs is the mainstay of treatment for Allergic Bronchopulmonary Aspergillosis (ABPA)?
- Steroids and itraconazole
- Fluconazole and albuterol
- Inhaled fluticasone
- Albuterol
- Inhaled racemic epinephrine
What finding in a complete blood count supports the diagnosis of allergic bronchopulmonary aspergillosis?
- Eosinophilia
- Leukocytosis
- Basophilia
- Neutrophilia
- Thrombocytopenia
Author of lecture Allergic Bronchopulmonary Aspergillosis (ABPA)

Brian Alverson, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
