Playlist
Show Playlist
Hide Playlist
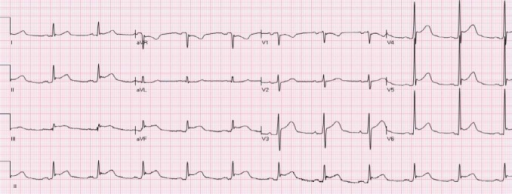
Acute Pericarditis: Signs and Symptoms

-
Slides Disease of Acute Pericarditis.pdf
-
Download Lecture Overview
00:01 Often will follow Upper Respiratory Tract Infection (URI) or myocardial infarction, usually be the fibrinous type pericarditis. 00:09 Or well, tell me about that. Remember post MI? And if it was days later? Fibrinous pericarditis. 00:16 What if it was three weeks and months later? Now you’re looking at autoimmune disease called dressler. 00:21 The cardinal symptoms: chest pain, describe as sharp or stabbing but not on the back. Is that clear? Stabbing back pain would be what? A dissection. 00:33 There’s a stabbing “Aw” in the heart. Relied sitting up and leaning forward. Relieved. 00:41 Relieved by sitting up and leaning forward because you cause further separation. 00:45 When did we last talk about this particular concept? It was dealing with the hypertrophic obstructive cardiomyopathy. Remember them. 00:50 The obstruction, the outflow track. What are you trying to do with outflow tract in HOCM? They’re trying to separate the two. What you trying to do here? To relieve that pain. You trying to separate the pericardial cavity. 01:02 You do that by leaning forward and exhaling. 01:06 Low grade fever, -itis; diaphoresis, tachycardia, tachypnea. 01:09 Because here, you might have decrease cardiac output, increase sympathetic activity resulting in the symptoms that you’re seeing here.
About the Lecture
The lecture Acute Pericarditis: Signs and Symptoms by Carlo Raj, MD is from the course Pericardial Disease: Basic Principles with Carlo Raj.
Included Quiz Questions
Which of the following statements about acute pericarditis is FALSE?
- It causes systolic dysfunction.
- Symptoms may present after an upper respiratory tract infection.
- It may be associated with acute renal failure.
- There is inflammation of the sac covering the heart.
- It may be a complication of myocardial infarction.
Author of lecture Acute Pericarditis: Signs and Symptoms

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
