Playlist
Show Playlist
Hide Playlist
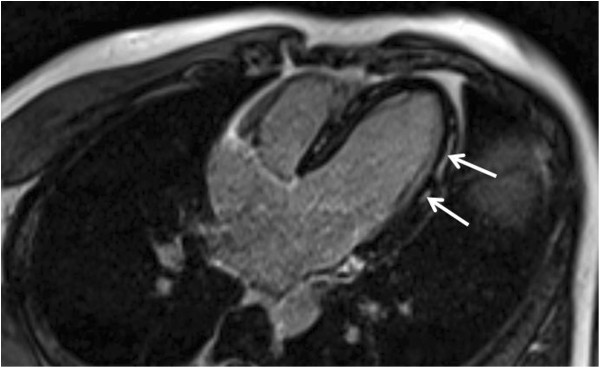
Acquired Myocarditis


-
Slides Endocarditis Myocarditis and Pericarditis Cardiomyopathy.pdf
-
Reference List Pediatric Nursing.pdf
-
Download Lecture Overview
00:01 So let's shift gears away from the endocardium into the myocardium or the muscle of the heart, and let's talk about acquired myocarditis. 00:11 Most acquired myocarditis is viral. 00:16 That's a pretty high-yield question right there -- Coxsackie B virus causing viral myocarditis. 00:22 Other viruses absolutely cause it, though, including adenovirus, hepatitis C, Epstein-Barr virus or cytomegalovirus. 00:30 Most viruses can cause it, Coxsackie B is the most common culprit. 00:37 COVID-19 virus can also cause acute myocarditis. 00:42 If myocarditis is not viral, it could be from another infection. 00:47 Examples of this are bacteria, for example, Rickettsial diseases can cause it. 00:54 Lyme disease can cause it -- remember Lyme disease is Borrelia burgdorferi. 00:58 And not seen so much in the United States but in South America, Chaga's Disease can cause it, and that's a protozoa. 01:05 There are also non-infectious causes of myocarditis: autoimmune or environmental. 01:13 Autoimmune diseases like Kawasaki Disease, rheumatic fever, collagen vascular disease can all cause inflammation of the myocardium. 01:21 And then very rarely, environmental causes exist as well, a variety of toxins and drugs. 01:27 But these other infectious causes and environmental and autoimmune causes are quite rare compared to the viral causes which are by far the most common. 01:37 When you think of viral causes you often think, "Well, it's gonna be a benign condition," but acquired myocarditis, even if viral, can be very, very dangerous. 01:49 These viral causes often causes fever, flu-like symptoms, and irritability in children. 01:55 If they get severe, they can go into congestive heart failure. 01:59 And they can have complete muscle failure of that ventricle which can cause all kinds of systemic problems. 02:06 They can develop dyspnea, they can have a poor appetite, they can have exercise intolerance. 02:13 You may notice hepatosplenomegaly or an S3 or an S4 on exam. 02:18 Remember, the S3 and the S4 are a resulting sound from a non-compliant stiff ventricle. 02:26 Well, if that myocardium is inflamed it's not gonna be very compliant. 02:30 These patients can develop arrhythmias because of irritation and interruption of the electrical system through the myocardium. 02:40 They may develop ventricular tachycardia or any degree of heart block that you can find on EKG. 02:47 They can also have an associated pericarditis and we'll talk about that in a bit, but you may hear a friction rub on exam if they have an associated pericarditis. 02:58 So you're worried about this. You obtain a chest x-ray and oftentimes a chest x-ray will just show a large heart. 03:05 You may have pulmonary vascular congestion if they're having some right-sided failure as well. 03:11 An EKG will show low voltage QRSes, and that's very important to remember. 03:19 The voltage on those QRSes across the board on that EKG are gonna be a lot lower as you can see in this picture. 03:25 Patients may have inverted T waves; they may have wide QRS complexes; and they may have ST-segment changes, and all of these are possible in acquired myocarditis. 03:39 The echo is really where you're gonna get at what the problem is and you can see visually on the echocardiogram that there's poor functioning of that myocardium. 03:49 If you suspect acquired myocarditis, we will often obtain viral serology, especially Coxsackie titers. 03:58 But you'all also get any other blood testing as indicated depending on what the suspected cause is as we discussed in the various causes. 04:06 But remember: Coxsackie and viral titer testing is usually obtained. 04:12 So, how do we treat it? Well, in cases of acquired myocarditis that are mild, it's mostly supportive therapy. 04:21 We may provide ionotropes and provide some afterload reduction, and there's some controversy about IVIg. 04:31 Most people use IVIg simply because we think it might help. 04:36 But when you look at the evidence it's somewhat controversial. 04:40 There's a Cochrane review showing not much benefit. 04:43 But then again, these patients are potentially so sick we worry they may get worse off an IVIg as indicated. 04:50 In severe disease, we may provide with a ventricular assist device or patients may require a heart transplant.
About the Lecture
The lecture Acquired Myocarditis by Brian Alverson, MD is from the course Pediatric Cardiology.
Included Quiz Questions
What is the most common cause of acquired myocarditis?
- Viral infections
- Hypersensitivity
- Giant cell myocarditis
- Celiac disease
- Juvenile Idiopathic Arthritis
Which of the following clinical manifestations is least likely in a patient with acute myocarditis?
- Deep tenderness at McBurney's point
- Flu-like symptoms
- Arrhythmias
- Hepatosplenomegaly
- Dyspnea
Author of lecture Acquired Myocarditis

Brian Alverson, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Excellent lecture as usual. I would have liked to see the epidemiology (and mortality) but the info concerning the ethology and clinical presentation is enough to raise the suspicion of myocarditis in a sick child.
