Playlist
Show Playlist
Hide Playlist
Abdominal Aortic Aneurysm: Management

-
Slides Abdominal aortic aneurysm Special Surgery.pdf
-
Download Lecture Overview
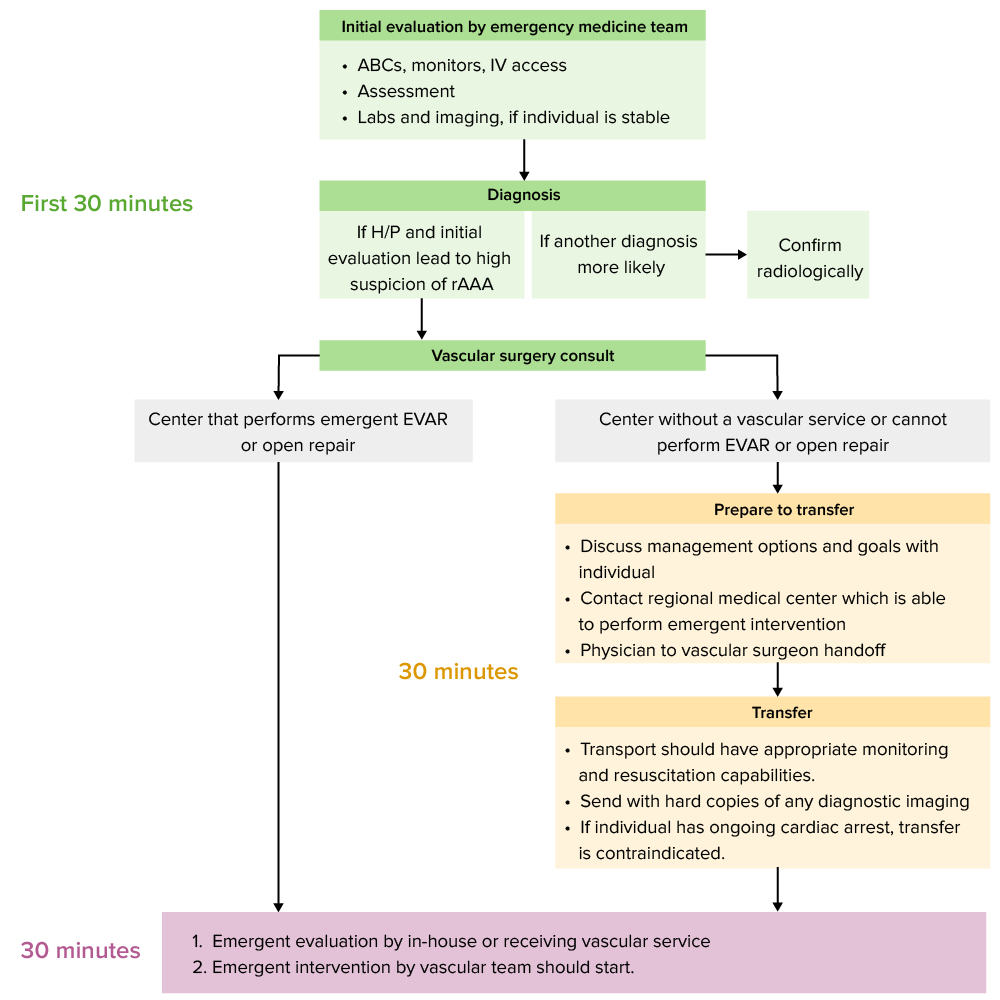
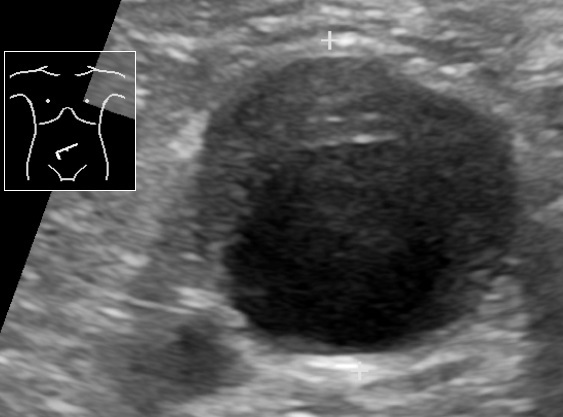
00:01 How do we manage Triple As once it's been diagnosed? Let’s start with medical management. 00:06 For patients who are asymptomatic - pharmacologic and lifestyle changes. 00:11 You know this to be a very common theme in peripheral vascular disease. 00:15 Pharmacologic, patients can be placed on anti-lipid therapy Statins again for plaque stability and antihypertensives. 00:24 Remember we talked about the wall stresses on the aorta? Beta blockers are particularly good at reducing wall stress and like all other vascular diseases lifestyle management is very important. 00:37 Number one, stop smoking and number two, weight loss. 00:41 This also reduces the likelihood of hypercholesterolemia and hyperlipidemia. 00:47 What are some indications for surgery? Remember, all symptomatic patients with Triple As require surgery. 00:54 Now, let’s discuss the asymptomatic patient. 00:57 Generally speaking, if the diameter of the abdominal aortic aneurysm is greater than 5.5 cm or it's actually growing faster then 0.5 cm per 6 month, these are potential indications for surgery. 01:12 The discussion has been for many years now, open versus endovascular techniques. 01:18 You may be familiar with the concept of endovascular techniques. 01:22 This is a hybrid open-access to the femoral vessels eventually using interventional radiology techniques to deploy a graft. 01:32 This is opposed to the tried and true open-method of opening the abdomen, accessing the aorta, removing the plaques and fixing the aneurysm. 01:42 Are there benefits and downsize to each? Of course there are. 01:46 Endovascular techniques is minimally invasive. 01:50 These are done quickly and the patients are usually out of the hospital within a day or two. 01:55 However, particularly in younger patients, endovascular techniques require lifelong surveillance, but it is associated with less perioperative morbidity. 02:07 In open-traditional technique, we know it to be durable. 02:11 It’s been tested over many decades and it may be more appropriate for young patients. 02:17 However, as previously described, it has a little bit more perioperative morbidity. 02:23 Once it’s decided the patient has indications for surgery, let’s discuss the surgical options. 02:30 We discussed how there's open and endovascular techniques. 02:33 Here on this image is an exposed open-abdominal aortic aneurysm repair. 02:39 You’ll notice that in the middle of the graft is already a graft placement of the previous aneurysmic sack. 02:46 Next, let’s take a look at an endovascular deployment. 02:50 To the left of the screen you see the initial insertion of the graft, this is done through the common femoral up to iliac through the common iliac into and pass the aortic sack. 03:03 And to the right of the screen, you see the aortic graft after deployment. 03:08 Remember, both open and endovascular techniques main goal is to bypass this aneurysmic sack. 03:16 This also restores laminar flow. 03:18 I’d like to post a question to you. When is screening necessary? I’ll give you a second to think about it. 03:26 Here’s some guidelines for screening from preventative societies. 03:30 First, any man aged 65 to 75 who have histories of smoking greater than 100 cigarettes per year with no family history of Triple As should be offered an ultrasound of the abdominal aorta. 03:42 Younger men between the ages of 55 and 75 who have a family history of Triple A can also be offered one. 03:51 Don’t forget, women also get Triple As even though there's a male preponderance. 03:56 Women between the ages of 55 to 75 who have both a smoking history of greater than a 100 cigarettes per year and a family of history of Triple A can be offered an ultrasound of the abdomen. 04:08 Women of any age who have neither smoking history nor family history of Triple A should not be offered screening as their incidence of an abdominal aortic aneurysm is low. 04:18 Now, let’s move on to important clinical pearls and high yield information. 04:23 Remember, any patient who presents with abdominal pain that has a known aortic aneurysm should prompt immediate work up for possible rupture. 04:33 And if the classic clinical scenarios presented to you or the patient comes in with searing abdominal pain radiating to the back, you should immediately prompt both work-up and management of an impending rupture. 04:46 Now, pay particular attention to this high yield information. 04:53 I like to post a clinical scenario to you. 04:56 What if two days after a Triple A repair, either open or endovascularly, you're called to the bedside because the patient now is presenting with bloody stools. 05:07 What’s going on in your mind and what are the differential diagnoses? How will you manage this? I’ll give you a second to think about this. 05:16 In this clinical scenario, it’s the classic description of ischemic colitis following a Triple A repair. 05:22 The reason behind this is the graft whether it’s placed endovascularly or open, likely covered up the inferior mesenteric artery. 05:32 s such, the inferior mesenteric artery is no longer supplying the sigmoid colon. 05:37 This can lead to ischemic colitis. 05:40 The work-up includes a flexible sigmoidoscopy to identify areas of ischemia and sometimes the inferior mesenteric artery actually needs to be re-planted. 05:52 Thank you for joining me on this discussion of Triple As.
About the Lecture
The lecture Abdominal Aortic Aneurysm: Management by Kevin Pei, MD is from the course Special Surgery.
Included Quiz Questions
Which of the following is an indication of surgery for an asymptomatic abdominal aortic aneurysm?
- 5.7 cm diameter of AAA
- 5.0 cm diameter of AAA
- 4.5 cm diameter of AAA
- 4 cm diameter of AAA
- 5.3 cm diameter of AAA
Which of the following groups do NOT require screening for AAA?
- Men aged 45 with a smoking history of >50 cigarettes per year and no family history of AAA.
- Men aged 60-75 with a smoking history of >100 cigarettes per year and no family history of AAA.
- Men aged >70 with a recent MI.
- Men aged 55-75 with a family history of AAA.
- Women aged 55-75 with a smoking history of >100 cigarettes per year and a family history of AAA.
Author of lecture Abdominal Aortic Aneurysm: Management

Kevin Pei, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
