Playlist
Show Playlist
Hide Playlist
Review

-
Slides Dehydration IntegratedRenalPathology.pdf
-
Reference List Pathology.pdf
-
Download Lecture Overview
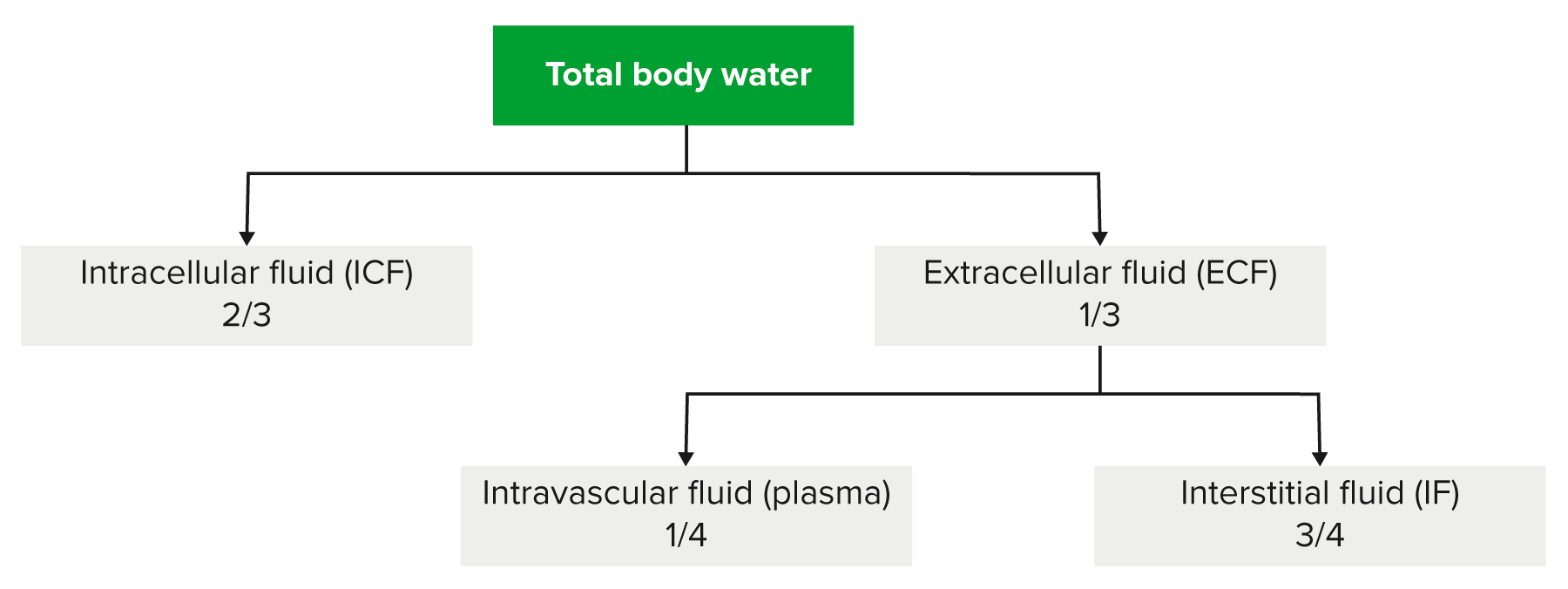
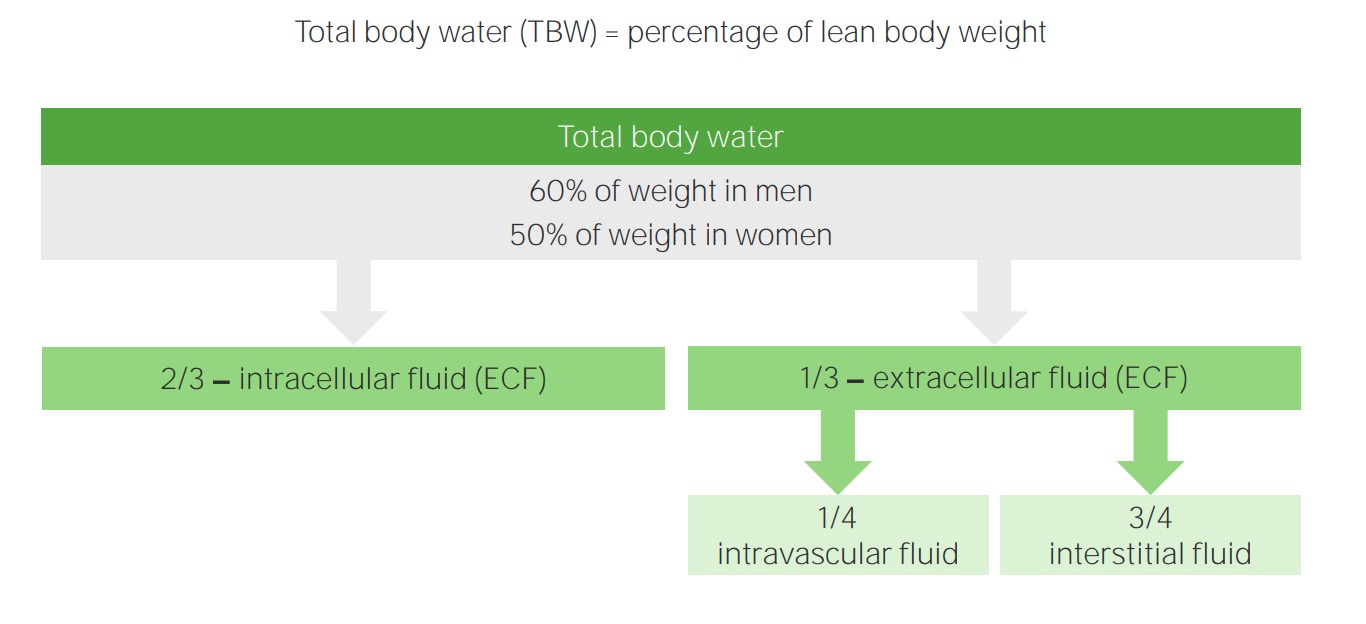
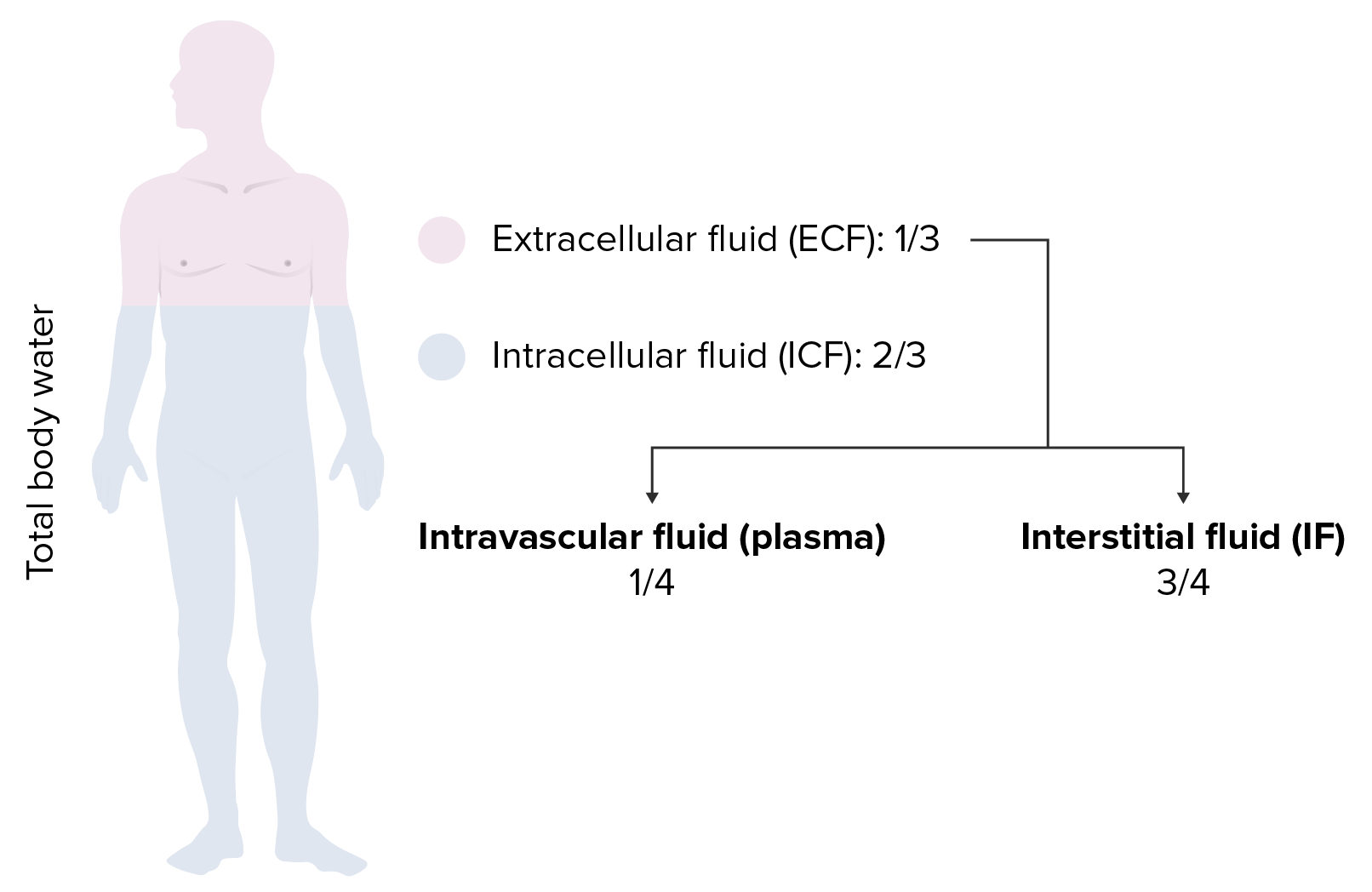
00:00 Quickly, we’ll walk through a table and we have completed our entire discussion of all disorders of water and sodium. This is strictly in terms of hypertonic. Let’s begin. I want us to take a look at the differentials in the last column with the conditions, DKA, hyperosmolar nonketotic coma, type 1, type 2 respectively, more commonly being presented. 00:25 So what’s happening? Let’s go to the box in the first column. You are having tons of urination. 00:33 Your ECF volume is going to decrease. You see that? A decrease in ECF volume, contraction, number one. Number two, take a look at that ECF osmolarity. I expect you to know at this point that small compartment that you’re seeing here in the box, what is that? ECF. 00:50 What's the bigger compartment in this box? The ICF, isn’t it? So now, the ECF volume decreases, ECF osmolarity increases. You pull the water out. ICF volume decreases. ICF osmolarity increases. 01:05 Bam! One two, three, four. Why is it that the sodium has been lost in this patient? Take a look at the second column. Why is it that sodium is decreased? Because you’re losing it. 01:15 What then is causing the increase in plasma osmolarity? Glucose. Good, let's so move on. 01:21 Hypertonic changes, continue our discussion. Now these, you can put them together because all of these are dependent on your sodium. The previous with DKA and such, that increase in plasma osmolarity was due to glucose, hence the separation. 01:38 You'll take a look at the last three issues here, all of them are dealing with sodium. Let’s begin. 01:45 We have osmotic diuresis and sweating, insensible water loss, diabetes insipidus, infusion of sodium. 01:52 I want us to do the trickiest one which is going to be osmotic diuresis. But Dr. Raj, didn’t we just do this with DKA? DKA, how bad is that? Worse case, late scenario of diabetes mellitus. What happens early on, early on in diabetes mellitus, in type 2 shall we say? What about sweating? What about sweating? I taste the salt but you're losing more what? Water, right, you're losing more water. 02:17 So, you'll find the following: In osmotic diuresis and sweating, you’ll have a decrease in total body water much greater than the loss in sodium. Is that clear? So therefore what happens to plasma osmolarity? Increases, increases, increases. You have contraction of both the ECF volume and ICF because you're literally losing the water. Next one, we have differentials insensible water loss from what? Fever and diabetes insipidus. What are you losing purely here? Water. 02:48 If all that you're losing is your denominator, what happens to your ratio? It increases. 02:54 Hence, an increase in plasma osmolarity. Would you please tell me why you would have normal skin turgor clinically with diabetes insipidus? Because the salt is unaffected, all that you’re doing is losing pure water. The last one is one in which we are literally taking in solute only, solute only. 03:17 So now you have sodium bicarb or perhaps, sodium containing-type of antibiotics. 03:23 What happens to your ECF osmolarity? It increases. You're going to pull the water out of the ICF, hence the volume contraction. ECF volume has expanded. Take a look at your ratio. 03:35 You find a crazy increase in total body sodium. Ratio increases, increase in plasma osmolarity. 03:42 Ladies and gentlemen, there is a lot of information here with both the tables. 03:47 Amazingly, wonderful, and beautiful differentials that you want to keep in mind so that you clearly know how your patient is presenting. You want to be quite familiar with this ratio of total body sodium over total body water. That is what determines your plasma osmolarity. That will then dictate the shifts of your fluid and volume between the ICF and ECF.
About the Lecture
The lecture Review by Carlo Raj, MD is from the course Fluid and Electrolyte Balance.
Included Quiz Questions
Which of the following scenarios would result in a contraction of the extracellular fluid?
- Overuse of diuretics
- Excess ADH
- Cushing's disease
- Infusion of Na-containing antibiotic
- Primary aldosteronism
Which of the following is least likely to show signs of volume depletion?
- Cushing syndrome
- Addisons disease
- 21 alpha hydroxylase deficiency
- Diabetic ketoacidosis
- Excessive sweating
Which of the following fluid compartment values MUST result in a fluid shift between the intracellular compartment and the extracellular fluid compartment?
- Change in plasma osmolarity
- Vascular compartment contraction
- Decrease in total body sodium
- Osmotic diuresis
- Interstitial fluid compartment expansion
Which of the following changes would you expect in a patient with a fever?
- Normal skin turgor
- Decreased plasma osmolarity
- ICF expansion
- Decreased total body sodium
- Increased total body water
Which of the following changes would you expect in a patient with type 2 diabetes?
- ECF volume contraction
- ICF volume expansion
- Hypernatremia
- ECF volume expansion
- Decreased plasma osmolarity
Author of lecture Review

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
