Playlist
Show Playlist
Hide Playlist
Zollinger-Ellison Syndrome

-
Slides Stomach and Duodenum.pdf
-
Download Lecture Overview
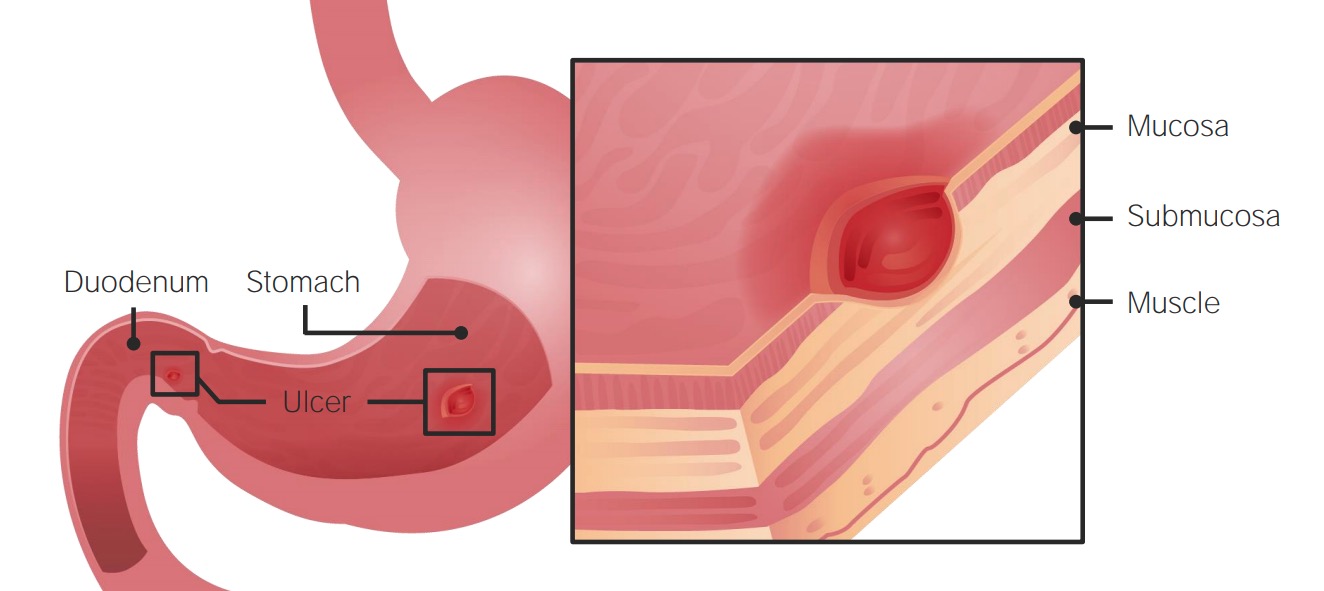
00:01 Take a look at ZE Syndrome, Zollinger−Ellison. In Endocrinology, our discussion of Zollinger−Ellison will be in greater detail. It’s a gastrinoma. And this gastrinoma is located in the pancreas perhaps. 00:16 It could be at organs as well and part of MEN−1. It’s a hypersecretion of gastrin from tumors in the pancreas or perhaps in the wall of the duodenum. It is a gastrinoma. How is it possible that you have a gastrinoma outside of the stomach when gastrin physiologically is coming out of the G cells of the antrum of the stomach? It’s a cancer, it’s a malignancy; it can do whatever it darn well pleases. 00:42 What are you looking for with ZE Syndrome? Ulcerations. Ulcerations not only in the stomach. Then you have, think of this of being like a lava when a volcanic eruption has taken place. When a volcano blows out lava, everything that it encounters in front of it is going to be obliterated. So here’s my acid that’s being produced in great quantity from your parietal cell. I don’t care where a gastrin is being released or where it’s coming from, it’s always going to work on your parietal cell. That’s where you form acid, period. So all these acids that’s being formed in great quantity will come out from the stomach into the duodenum and kill everything in it’s path. 01:26 So you might have issues of gastric ulcers, duodenal ulcers. Have you studied separately peptic ulcer disease of the jejunum? No. Peptic ulcer disease either in the gastric or in the duodenum. But if you, by chance, look for or your symptom description of an ulcer down in the jejunum, high on your differential should be gastrinoma or Zollinger−Ellison. Is that clear? Now there’s also diarrhea that is involved, the secretory type, because you’re producing all these acid. Malabsorption is a huge problem and refractory to treatment. Diarrhea due to secretion of all that gastric acid. Because there’s malabsorption, you can't properly take up your lipids because the, what are these fingerlike projections in the duodenum? They are called microvilli. And by Chemistry and Physiology, you have dealt with quite a bit and we have as well in hyperlipidemia with vascular pathology with the proper handling of your lipid. If the Brush border had been blunted or had been completely destroyed, then maybe lipid then starts accumulating in your stool, steatorrhea. Association with MEN−1. Once again with MEN−1, PAN-pancreas most likely where you would find this. 02:48 Parathyroid; PIT–pituirary with a prolactinoma; Part of MEN−1. 2/3rd of your gastrinomas are malignant tumors. 03:00 Majority are. ZE, your serum gastrin levels will be ridiculously high as will be the acid. That is not normal. 03:09 Whenever your acid levels are high, physiologically it tells my G cells to shutdown. So my gastrin levels should be low or with that increased levels of acid, somatostatin will tell my G cells to no longer release gastrin, I have enough acid. So you do have physiologic feedback normally. However, in ZE, please understand that that high levels of acid will not shut down the gastrin because the gastrin, this is a malignant tumor. 03:40 An important integration between physiology and pathology is the next statement. Secretin. Acids coming out, physiologically, from the stomach and into the duodenum. Acid into the duodenum. That pH in the acid or in the stomach is maybe at a pH of 2. Coming in to the duodenum, that’s dramatic. Yeah, and it is absolutely. It’s lava coming in to duodenum. So therefore the duodenum is now incredibly sensitive to this acid. It wants to do everything in its power to neutralize this acid as quickly as possible. What is the neutralizer for this acid in the duodenum? Bicarb. Where is the bicarb coming from? Pancreas. So give me the hormone that’s responsible for stimulating the pancreas to secret the bicarb into duodenum. 04:46 That’s your secretin, right? That’s your normal physio. Let’s take a look at what happens here in ZE and how you will utilize a physiologic Secretin test to help you diagnose ZE. The Secretin Stimulation Test needed for gastrin levels less than 1000. Positive test shows lack of gastrin suppression by administration of secretin. In other words, the secretin stimulation they're needed to gastrin levels less than 1000. 05:19 So want this so that you can decrease the gastrin. If the secretin comes out and the gastrin levels are still high, this is going to then help you diagnose ZE. 05:31 Further, you want to localize the tumor by using octreotide scan. You’ll do what’s known as a ultrasound so that you can properly localize your tumor. A CT scan, angiography and surgical exploration, well, all of them help you properly identify your tumor so that you can then excise it. Remember, you can manage it by using certain drugs. However, in order for you to cure your patient you have to resect this tumor. 06:07 What you’re seeing here is the fact that you are destroying everything in the path of your intestine. 06:19 So as acids coming in, as you see the cartoon here, you’ll notice the duodenum with scattered, scattered, scattered ulcers, completely refractory to any type of treatment. H2 blocker or your PPIs. 06:32 All should indicate that your patient maybe is suffering from ZE. I've gave you some diagnostic tools including the fact that hypergastrinemia is present, the secretin test is not effective or shows that the gastrin levels are still high and number three, the basal output. Management. High dose of PPI. 06:55 Surgical resection, if no metastasis or not associated with MEN−1. Parietal cell vagotomy for gastric hypersecretion. 07:05 Chemotherapy for metastatic disease. It’s important that you pay attention to the normal feedback mechanism because the angles in which they could possibly ask you, experimentally, for ZE is every possibilty because this could be a wonderful pathophysio question in which if you know that there’s too much acid coming into parietal cell then you should be thinking about all the different receptors that you have on there including gastrin receptors for secretion, your H2 receptor for secretion, your PP on the luminal side. 07:35 And the fact that you have an M3 receptor, referring to my vagal tone, right. Or in other words, your vagus in parasympathetic.
About the Lecture
The lecture Zollinger-Ellison Syndrome by Carlo Raj, MD is from the course Stomach and Duodenum Diseases: Basic Principles with Carlo Raj.
Included Quiz Questions
Which of the following is common in patients with Zollinger-Ellison syndrome?
- Steatorrhea
- Rectal prolapse
- Pale stools
- Jaundice
- Constipation
What fraction of gastrinomas are malignant tumors?
- Two-thirds
- One-fourth
- Three-fourths
- Two-fifths
- One-eighth
What is the gastric pH in Zollinger-Ellison syndrome?
- < 2
- > 2
- > 4
- > 5
- < 1
Which of the following is NOT a localization test for Zollinger-Ellison syndrome?
- Serum gastrin level
- CT scan
- Angiography
- EUS
- Octreotide scan
Author of lecture Zollinger-Ellison Syndrome

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Excellent, very detailed, now feel more confident in the treatment and care of this infection
