Playlist
Show Playlist
Hide Playlist
Lymphadenopathy: Thymus Disorders – White Blood Cell Pathology

-
Slides Lymphoid Tissue Thymus White Blood Cell Pathology.pdf
-
Download Lecture Overview
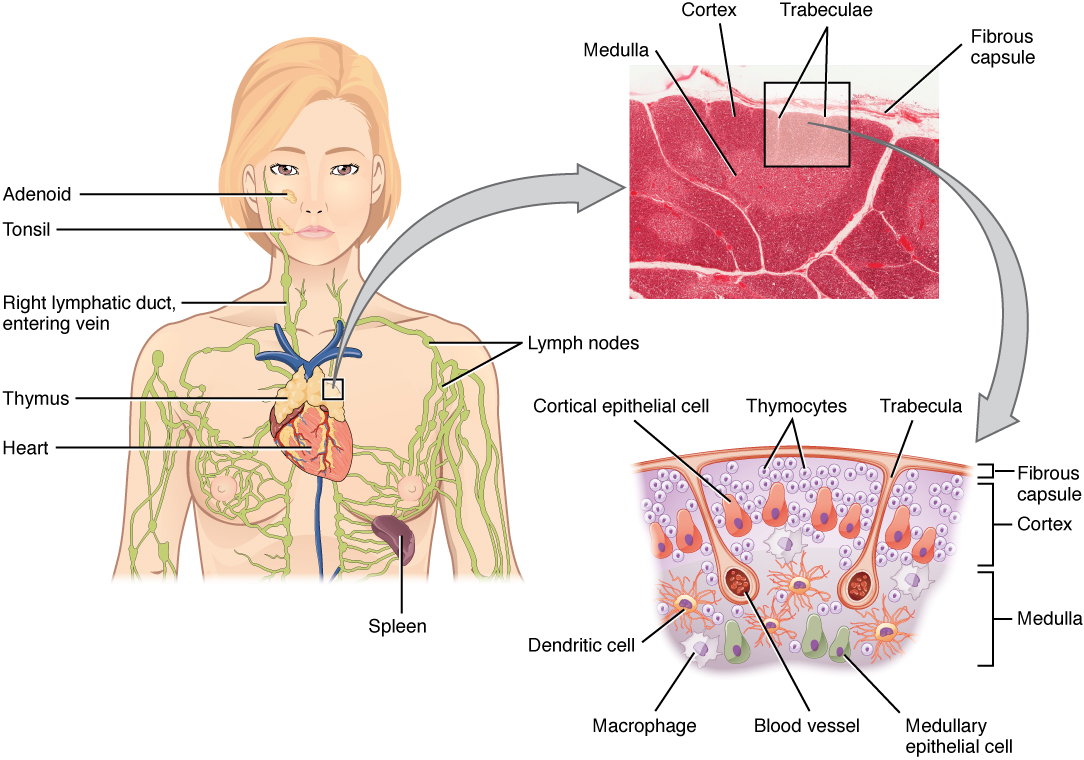
00:01 The way to approach thymic pathology in this section would be, well, is the thymus present? So maybe perhaps thymic hypoplasia or is there too much thymus activity. 00:15 Let’s take a look. 00:17 First, we’ll take a look at a congenital disorder that you should be quite familiar with in which, literally, the thymus does not form. 00:26 This obviously is going to bring you to a topic of DiGeorge. 00:30 So DiGeorge syndrome as you see in the picture here is showing you that the third and fourth pharyngeal pouches, which are normally responsible for developing the superior and inferior parathyroids and then also the third pharyngeal pouch, not only does it give rise to your inferior parathyroid, but it will also give rise to your thymus. 00:49 And the DiGeorge syndrome, as you know, chromosome 22, long arm 11, that you don’t have this. 00:57 Abnormal development of third and fourth pharyngeal pouches, loss of the thymus, now how’s your patient presenting? Well, you know about recurrent infections. 01:08 Recurrent infection has a long list of differentials including DiGeorge, including your Chédiak-Higashi, including chronic granulomatous disease, including Bruton's agammaglobulinaemia, Wiskott-Aldrich, the list goes on and on and on. 01:22 And those become important in immunology. 01:25 Here, if the thymus is not present, then your patient is most likely susceptible more so to viral infections, but you know the peculiar symptom that you’re going to find here that you would in other conditions, that have recurrent infection will be the fact that if for example, if you placed pressure or if you snapped on your facial nerve, that you would have Chvostek sign, or in other words, you're eliciting tetany or perhaps a cuff around the arm and therefore resulting in carpopedal spasms or oral mucosa type of numbness, right? All of these put together with DiGeorge Syndrome and just to be complete, that chromosome 22q11, you’ve heard of velocardiofacial issues. 02:15 That becomes important in embryology. 02:17 Spend a little bit of time with that chromosome 22, what may then happen if that gets deleted? Not only could it be DiGeorge, but another condition that’s important called velocardiofacial abnormality. 02:29 Here, our topic is hyperplasia, thymic, follicular hyperplasia, why does this occur? Occurs in chronic inflammation in immunologic states. 02:40 Remember what the thymus is responsible for in a child. 02:43 Obviously, as an adult, our thymus gets involuted, apoptosis. 02:48 We don’t have a significant thymus. 02:49 We shouldn’t and that’s important. 02:52 At some point, I’ll walk you through another set of diagnosis called thymomas, okay? But here, it’s the thymic hyperplasia. 03:00 Remember that thymus is responsible for proper education of your T-cells. 03:05 So T-cells are being born out of your bone marrow, they then come to your thymus, for proper education. 03:11 In other words, to make sure that you get rid of the self T-cells. 03:15 Frequently accompanied by myasthenia gravis. 03:16 We’ll talk about this in greater detail. 03:19 Oftentimes, you’ll find thymus in which it undergoes hyperplasia, which may then be called a thymoma. 03:25 I’m setting you up as to what’s to come.
About the Lecture
The lecture Lymphadenopathy: Thymus Disorders – White Blood Cell Pathology by Carlo Raj, MD is from the course Lymphadenopathy – White Blood Cell Pathology (WBC).
Included Quiz Questions
Which of the following is associated with DiGeorge syndrome?
- 22q11 deletion
- 15q11deletion
- 5p-deletion
- SMN1 deletion
- 15q13deletion
Which structures must undergo abnormal development to cause agenesis of the thymus?
- Third and fourth pharyngeal pouches
- First and second pharyngeal pouches
- Second and third pharyngeal pouches
- Second and fourth pharyngeal pouches
- Fourth and fifth pharyngeal pouches
What is the clinical sign that consists of carpopedal spasm due to the inflation of the sphygmomanometer cuff?
- Trousseau's sign
- Carnett's sign
- Babinski sign
- Aaron sign
- Chvostek sign
Author of lecture Lymphadenopathy: Thymus Disorders – White Blood Cell Pathology

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
very interesting lectures , lots of information, summarized , therefore easy to remember and to be applied in practice
