Playlist
Show Playlist
Hide Playlist
Primary Amenorrhea: Causes

-
Slides Primary and Secondary Amenorrhea.pdf
-
Download Lecture Overview
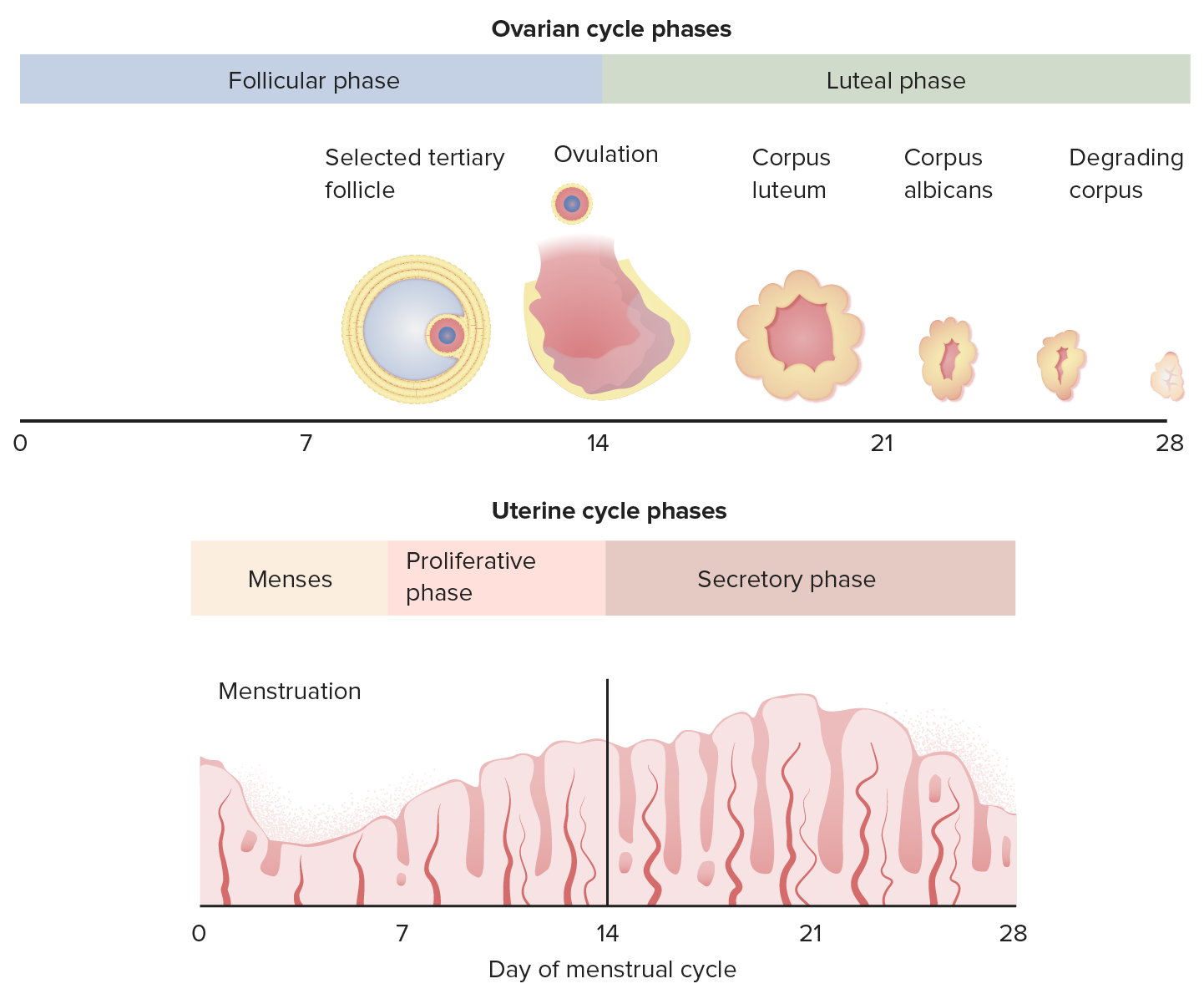
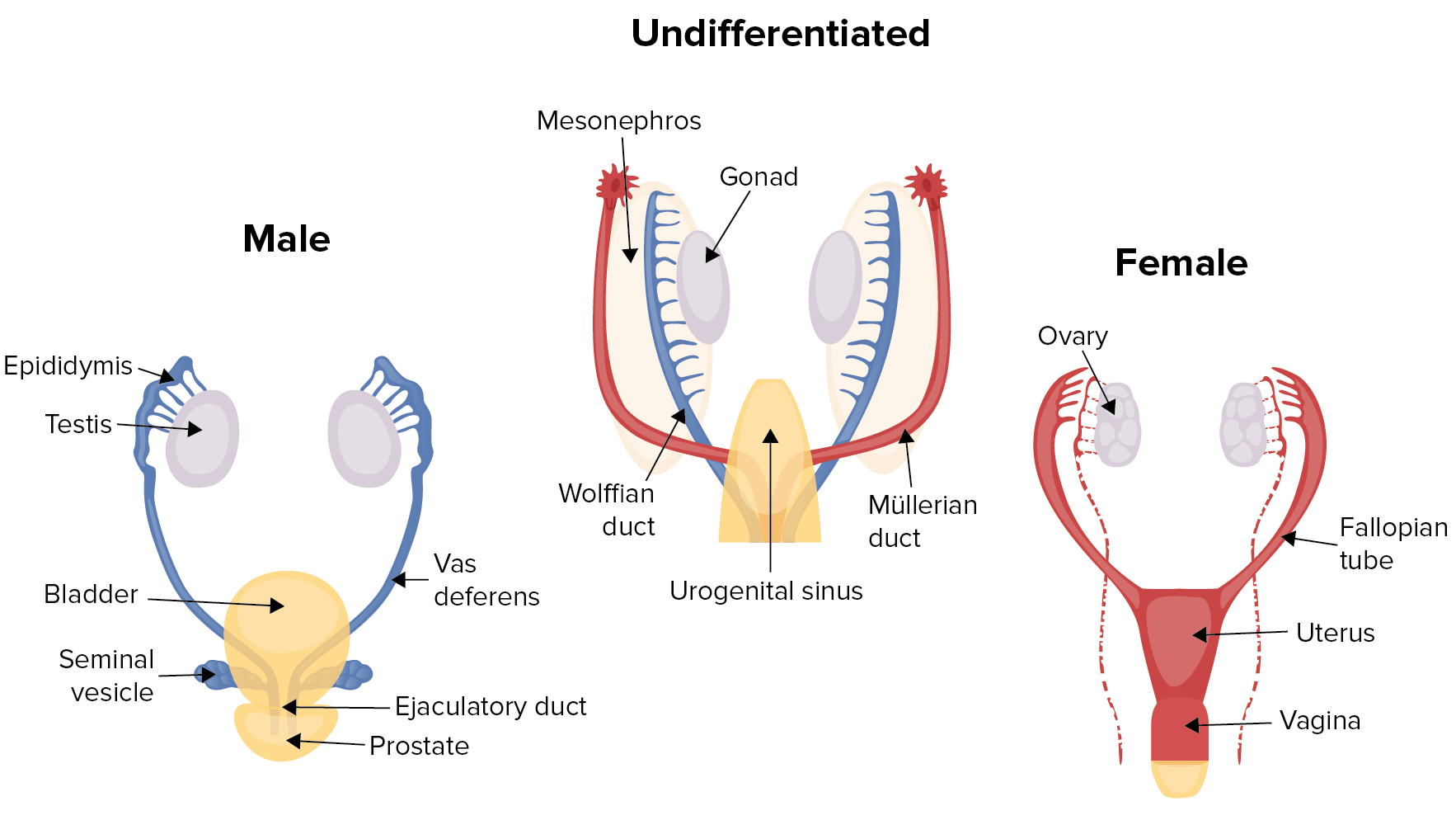
00:00 Hello. I would like to discuss primary and secondary amenorrhea with you. This is often tested on the USMLE so pay close attention. Let's review what a normal menstrual cycle is like. It's between 21 and 35 days. There is another lecture about AUB if you'd like to find out more. I'd like to discuss the terminology that we use. Oligomenorrhea means periods that are greater than every 35 days apart. It can also mean less than 9 menstrual cycles per year. Polymenorrhea is different. It actually means that your periods come too frequently. They are less than 21 days in the intermenstrual bleeding. Menorrhagia means you have too much flow greater than 80 mL in 7 days. Metrorrhagia means that you have a regular bleeding between menses. Amenorrhea means no menses, that can be either primary or secondary and we'll find out more in just a second. 01:07 Dysmenorrhea is defined as painful periods. 01:11 There are two types of dysmenorrhea with primary dysmenorrhea, and you have painful menstruation in the absence of any pelvic pathology. 01:20 Primary dysmenorrhea characteristically begins when adolescents attain ambulatory cycles, meaning they start to actually ovulate because you don't always ovulate at the beginning of menarche. 01:31 Usually this occurs within six to 12 months of menarche. 01:36 Secondary dysentery refers to painful menses due to pelvic pathology or a recognized medical condition. 01:45 Such as endometriosis, which is the most common cause. 01:48 Let's talk now about AUB classification. 01:52 This is a newer classification, and it starts with AUB, AUB/HMB which is heavy menstrual bleeding, which was formerly referred to as menorrhagia. 02:02 Intermenstrual Bleeding, which was formerly referred to as metrorrhagia. 02:08 Remember, if you'd like to know the new terminology please refer to the AUB lecture. So this is an overview of the hypothalamic pituitary axis. Now depending on what the target organ is, there are different hormones that come from the hypothalamus. There are different hormones or gonadotropins or tropic hormones that come from the anterior pituitary and the posterior pituitary and they have different effects on the target organ. All of these systems may have a role in normal menstrual cyclicity. You can see here the target end-organ hormone production is definitely influenced by the anterior pituitary and the pituitary. Let's review primary amenorrhea. In primary amenorrhea, you have never had a menstrual cycle. This is pathologic if you are age 13 and have no secondary sexual characteristics. To remind you, breast, axillary, and pubic hair are all secondary sexual characteristics. By age 15, even if you have secondary sexual characteristics if you have no menses this is pathologic. Again, it's very important to remember that the HPO axis must be intact for young woman to have a menstrual cycle. If she has amenorrhea, something has gone wrong at the level of the HPO axis. It could be the environment that is feeding back information into the CNS. The CNS then obviously corresponds to the hypothalamus. The hypothalamus has to release gonadotropin-releasing hormone to the anterior pituitary. The anterior pituitary will release gonadtropins, FSH, follicle-stimulating hormone, and luteinizing hormone or LH to the ovary. The ovary then produces estrogen and progesterone. The uterus is influenced by estrogen and progesterone and the withdrawal of both of those hormones result in a menstrual cycle. Let's now go over the common causes that we see in primary amenorrhea. If you have a patient that has breast development, you should consider that their cause of primary amenorrhea may be Mullerian agenesis. There is a separate talk on Mullerian agenesis or variance in another lecture if you'd like more information. Also, androgen sensitivity can also present as primary amenorrhea. There is another lecture set where you can learn more about complete and partial androgen sensitivity. Also, women may have anatomic factors that actually prevent menses. One of those is a vaginal septum. They may also have an imperforate hymen or they may overall have constitutional delay. If you have no breast development, likely you will have a high FSH or follicle stimulating hormone. This can happen in normal genetic female such as 46,XX. It can also happen in 46,XY individuals. Let's also now talk about low FSH. You can typically have a low FSH with constitutional delay. This also happens with prolactinomas and Kallmann syndrome. You may get tested about Kallmann syndrome so I will spend a little time here. These patients usually have anosmia which means they cannot smell. 05:39 They usually have primary amenorrhea and will need assistance to become pregnant should they like to become pregnant in the future. Other CNS pathology can also lead to a low FSH. Stress, weight loss, and anorexia is typical to have a low FSH associated with it. Polycystic ovarian syndrome can also have a normal to low FSH and again congenital adrenal hyperplasia may have a low FSH as well. If you'd like to learn more about CAH or congenital adrenal hyperplasia, there is a separate lecture set for that. I want to bring your attention to a really quick mnemonic to remember the causes of primary amenorrhea. When I was a medical student, it was difficult for me to remember but I'm going to give you a quick tip on how you can remember it. Remember XMAS. 06:29 X is for 45,XO or monosomy associated with Turner syndrome. M is for Mullerian agenesis. Recall that there is another lecture about Mullerian agenesis that you can review. A is for androgen insensitivity syndrome. This is typical with complete androgen insensitivity syndrome. Again, you can review this in another lecture set. Lastly, S is for Swyer syndrome. This is also referred to as XY gonadal dysgenesis.
About the Lecture
The lecture Primary Amenorrhea: Causes by Lynae Brayboy, MD is from the course Abnormal Menstruation. It contains the following chapters:
- Primary Amenorrhea
- Causes of Primary Amenorrhea
Included Quiz Questions
Which of the following is the term used in a patient who has lost 200 ml of blood over a 7-day menstrual cycle?
- Menorrhagia
- Metrorrhagia
- Polymenorrhoea
- Amenorrhea
- Dysmenorrhea
Which of the following best describes polymenorrhea?
- Menstrual intervals less than 21 days
- Menstrual intervals greater than 35 days
- Excessive menstrual blood flow
- Irregular bleeding between menses
- Pain during menses
Which of the following scenarios would be considered pathological for a patient with primary amenorrhea?
- A 13-year-old girl who has never had menses and no development of secondary sexual characteristics.
- An 11-year-old girl who has never had menses and no development of secondary sexual characteristics.
- A 13-year-old girl who has never had menses but has development of secondary sexual characteristics.
- An 11-year-old girl who has never had menses but has development of secondary sexual characteristics.
- A 14-year-old girl who has had menses only once and has development of secondary sexual characteristics.
Which of the following is NOT a cause of primary amenorrhea?
- Asherman syndrome
- Swyer syndrome
- Turner syndrome
- Androgen insensitivity syndrome
- Mullerian agenesis
Author of lecture Primary Amenorrhea: Causes

Lynae Brayboy, MD
Customer reviews
4,7 of 5 stars
| 5 Stars |
|
2 |
| 4 Stars |
|
1 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Hello Dr.Lynae Brayboy,good lecture,keep it going!All the very best!
Hi, just curious as to why a video like "Normal Menstrual Cycle" is all the way at the bottom? The ordering of this entire gynae course, not just this "Abnormal Menstruation" section (which again, is the first section on the contents page), makes navigating and understanding the content more difficult. Would it be possible to re-order them?
Clarity, specificity, definitive, flawless style, overall lecture is eloquently delivered.
