Playlist
Show Playlist
Hide Playlist
Lymphadenopathy: Plasmacytoma, MGUS and Lymphoplasmacytic Lymphoma – White Blood Cell Pathology

-
Slides Lymph Nodes.pdf
-
Download Lecture Overview
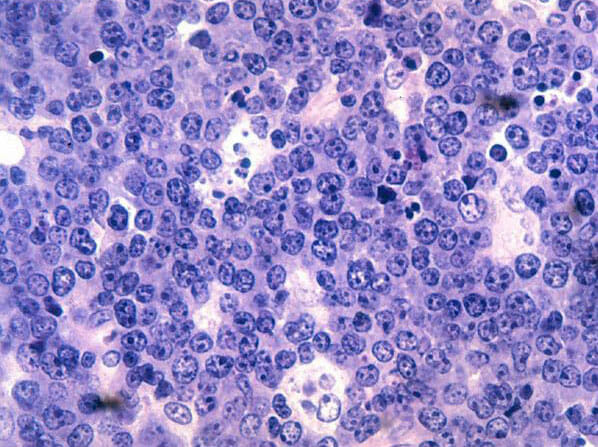
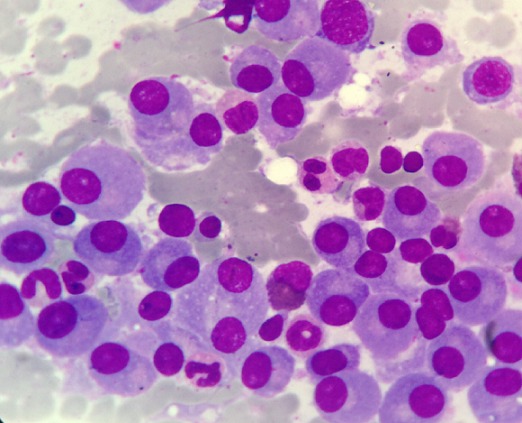
00:01 Our topic here is, “Plasmacytoma.” Plasmacytoma could be solitary, a lesion, consisting of once again monoclonal neoplasms of the plasma cell, so, we have a monoclonal gammopathy. 00:13 With solitary, one lesion, would be perhaps in the bone marrow, intramedullary or if it's extramedullary, the number one location for extramedullary type of plasmacytoma solitary type, would be the upper respiratory tract. 00:34 Solitary lesion type of plasmacytoma: Bone marrow, extramedullary, upper respiratory tract. 00:41 Then you have bony plasmacytomas, usually eventually present into or lead into multi-myeloma, 10 to 20 years down the road. 00:52 So, you have your solitary lesions or solitary plasmacytoma, which could be intermedullary or could be extramedullary, and then the bony plasmacytomas, may then go on to multi-myeloma decades down the road. 01:06 Extraosseuous plasmacytoma rarely progress, and can often be surgically cured. 01:13 Okay, make sure that you know the different patterns of plasmocytomas, this is once again you have a monoclonal gammopathy, from the plasma cell but it could be solitary, it could be within intramedullary/extramedullary, it could be bony or it could be extraosseuous, which could be surgically cured. 01:34 Our topic here is MGUS, which stands for: Monoclonal Gammopathy of Undetermined Significance. 01:40 So yet, we have another monoclonal gammopathy. 01:43 You have an M protein, so, this would rather seem like it would be multi-myeloma you actually find IGG or IGA, but guess what? Luckily with MGUS, there are no other bony infiltrative type of symptoms in your patient. 02:01 So, there is no bone pain and as far as signs, no pathologic fractures, there's no hypercalcemia, no hypocalciuria, so and so forth, found in 1% of people greater than 50, incidence would increase with age, and only a small percentage may then go on to multi-myeloma. 02:20 So MGUS, quite common, it is actually the most common monoclonal gammopathy, you might find an M protein, you might find a gamma spike, with IGG or IGA, but you will not find punched lesions, that to you ladies and gentlemen should be, MGUS. 02:36 Monoclonal Gammopathy of Undetermined Significance. 02:42 Here we have, Lymphoplasmacytic Lymphoma. 02:46 A plasma cell neoplasm. 02:48 I asked you earlier when you go through this, comparing contrast lymphoplasmacytic lymphoma, with multi-myeloma. 02:55 Let's do this now. 02:57 Multi-myeloma is a plasma cell issue, obviously, but the problem arises from the bone marrow. 03:04 There's every possibility with multi-myeloma, which arises from the bone marrow, to enter the lymph node, and look like a lymphoma, don't forget that, ever! So, just because you have a disease, or a cancer that begins in the bone marrow, doesn't mean that it wouldn't present as a lymphoma, it very well could. 03:22 Here however, with Waldenström macroglobulinemia, it actually begins in the lymph node, so, it's a lymphoplasmacytic lymphoma. 03:32 What is a plasma cell primitively or, what cell differentiated into a plasma cell? A B-cell. 03:40 So, if you're thinking about a lymph node, in which you have a cancer that is developing into a plasma cell, then you have to be referring to the B-cell, welcome to Waldenström. 03:49 So Waldenström consists of neoplastic B-cells, where are you? In your lymph node. 03:55 Not necessarily plasma cells, that secrete monoclonal IgM, interesting isn't it. 04:02 What's the immunoglobulin that you're producing here? IgM, Waldenström, IgM. 04:10 I asked you earlier, when we began the section of plasma cell dyscrasia, about the size of your IgM. 04:16 It's the biggest immunoglobulin, it is a pentamer. 04:20 And imagine your patient secreting abundant IgM into circulation, or gets into circulation, all this IgM which is now aggregating, this is not good, in other words, you've heard of hyperviscosity syndrome, hyperviscosity syndrome mind you, could also be found in multi-myeloma, but predominantly found with Waldenström, kind of like when we did our DKA, “Diabetic Ketoacidosis Acidosis,” predominantly found in type 1 as being uncontrolled, but could also be found in type 2. 04:57 Hyperviscosity syndrome, predominantly found in Waldenström, could also be found in multi-myeloma, keep that in mind, especially because of IgM, the pentamer. 05:08 Next, so if there's hyper viscosity, how is a patient presenting? The increased immunoglobulin levels in the blood, change its physical consistency, to one that's more thick and viscous. 05:18 This hyper viscosity hinders the blood's ability to flow freely, through the small arterials, and ultimately prevents adequate tissue perfusion from multiple organ systems. 05:28 There will be visual disturbance, there'll be neurologic issues, maybe stroke-like symptoms, or there is going to be bleeding. 05:35 Now, Waldenström macroglobulinemia, would you have such major bone lytic lesions, not so much, not so much. 05:46 Patients also present with hepatomegaly, lymphadenopathy and anemia, with modern treatment options this disease has an indolent course, and the median patient survival is now longer than 10 years. 06:00 Now, at this juncture, I kindly ask you to compare and contrast Waldenström, with your multi-myeloma. 06:07 You do that first, as far as your priorities, once you've understood/defined differences between those two, then you take a look at, monoclonal gammopathy of undetermined significance, and do not forget about plasmacytomas, the solitary type, and what it means to be within the medulla, and extramedullary. 06:26 You go in that order, and you keep your thoughts nice and organized, with plasmas and neoplasm, there is no way that the boards will trick you. 06:34 If you just look at everything at once and start memorizing, things become a little bit more difficult. 06:42 A picture here, is showing you “Rouleaux Formation.” I want to tell you that this is a non-specific finding, you're not going to find this only with multi-myeloma, you're not going to find this only with Waldenström, you could find it with a monoclonal gammopathy, so, what's happening? It's physics, so I'm not going to go into great detail, you're not going to be asked by the question, about the pathogenesis of rule formation, my goodness, but be able to identify it, and know where in terms of family of diagnosis you are. 07:15 You see rouleaux formation, in terms of family, you should be thinking about plasma cell dyscrasia, that's it, now it's because of the charges, just to make sure we're complete, because remember, Waldenström or multi-myeloma, you're producing IGG, IGG is being produced by which plasma cell dyscrasia? Good, multi-myeloma. 07:37 IgM Waldenström, point is, lots of immunoglobulin, you mess up the charges, and the charges here are then going to attract RBC’s, literally stacking up on top of each other like poker chips. 07:52 Poker chips, hence it's called rouleaux formation.
About the Lecture
The lecture Lymphadenopathy: Plasmacytoma, MGUS and Lymphoplasmacytic Lymphoma – White Blood Cell Pathology by Carlo Raj, MD is from the course Lymphadenopathy – White Blood Cell Pathology (WBC).
Included Quiz Questions
Where are extramedullary plasmacytomas most often located?
- Upper respiratory tract
- Lower respiratory tract
- Ribs
- Bone marrow
- Thoracic and lumbar vertebrae
Which of the following is the most common monoclonal gammopathy?
- Monoclonal gammopathy of undetermined significance
- Extramedullary plasmacytoma
- Lymphoma
- Multiple myeloma
- Solitary plasmacytoma of bone
Which of the following is NOT usually seen in monoclonal gammopathy of undetermined significance?
- Punched out lesions
- Gamma spike with IgG
- M protein
- Gamma spike with IgA
- Monoclonal paraprotein band
Which of the following presents with hyperviscosity syndrome?
- Waldenstrom macroglobulinemia
- Hodgkin's lymphoma
- Solitary plasmacytomas
- Non-Hodgkin lymphoma
- Multiple myeloma
Author of lecture Lymphadenopathy: Plasmacytoma, MGUS and Lymphoplasmacytic Lymphoma – White Blood Cell Pathology

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
