Playlist
Show Playlist
Hide Playlist
Parkinsonism and Treatment of Parkinson's Disease

-
Slides 03 AnomaliesAgingBrainParkinsonHuntington Aging.pdf
-
Download Lecture Overview
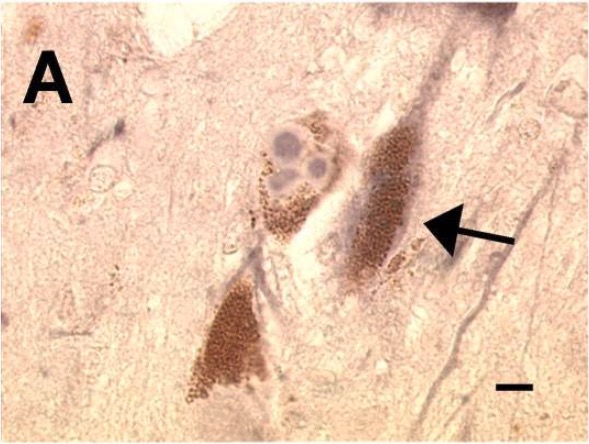
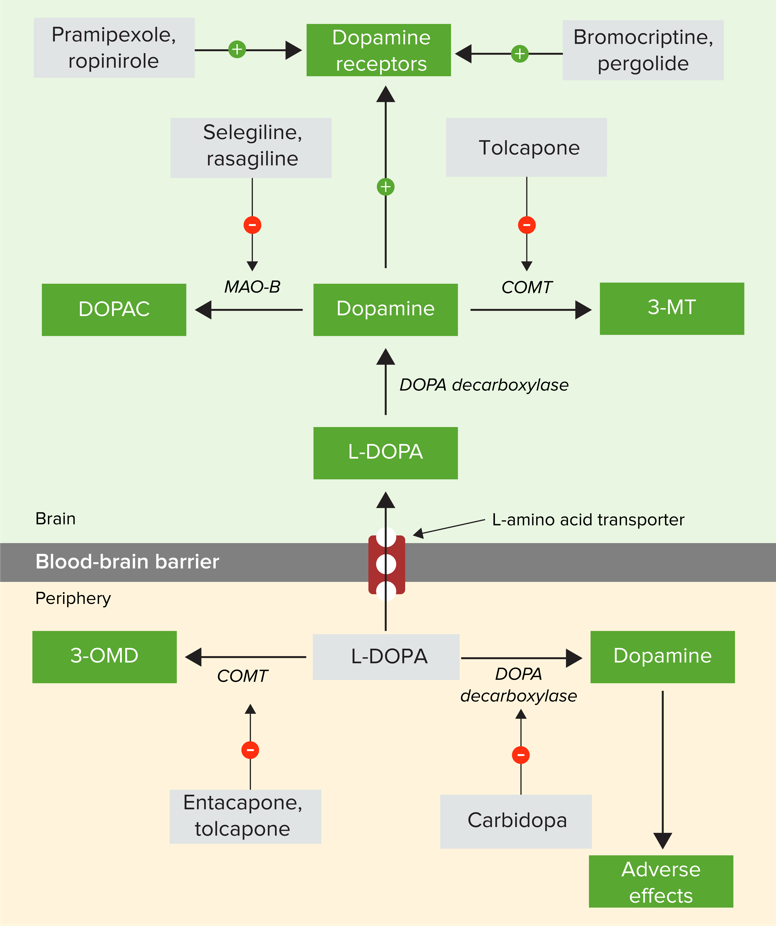
00:01 Let’s look at Parkinsonism versus Parkinson’s disease. Parkinsonism is a syndrome of Parkinson-like symptoms. That’s something that you need to keep straight. 00:17 Parkinson’s disease is not the only cause of these types of symptoms. So, we consider Parkinsonism separate from Parkinson’s disease. There is primary Parkinsonism which is a result of Parkinson’s disease and the classic Lewy body and neural degeneration. Then other versions of Parkinsonism, we consider as secondary Parkinsonism, so things that develop from non-Parkinson’s disease syndromes. 00:55 When we treat Parkinson’s disease, there are a number of different options. First of all, L-DOPA. 01:08 Historically, L-DOPA has been around for much longer than it was actually used for treatment of Parkinson’s. 01:15 It was initially used in the treatment of heroin withdrawal symptoms. It turns out heroin withdrawal symptoms have some of the same characteristics and difficulty of initiating movements and tremors that we see in Parkinson’s disease. So, someone thought let’s try this out on Parkinson’s patients. 01:37 It worked. So, that was great progress. However, it didn’t work forever, right? The effect of treatment with L-DOPA even with increasing doses didn’t resolve the symptoms. But initially, L-Dopa on its own would relieve some of the early symptoms of Parkinson’s disease. Now, how does L-DOPA work? It turns out L-Dopa or levodopa is a precursor to dopamine. So, it also crosses the blood brain barrier. 02:11 So, it can be taken orally, crosses the blood brain barrier at which point it is converted into dopamine. 02:18 Now, it can also be converted into epinephrine and norepinephrine which can have its own issues. 02:25 But the dopamine here is essentially adding extra dopamine so that the lower number of neurons have more signal being thrown at them and can make some signals. This works. 02:39 Dopamine functions return and things look good for a while. But the issue comes in that L-DOPA also can be converted in the peripheral nervous system. Here, perhaps the epinephrine and norepinephrine create some adverse effects. So we have additional dopamine in areas and norepinephrine and epinephrine in areas where it’s not necessarily needed. In order to alleviate some of these symptoms, what we now do is L-dopa should be coadministered with a dopa decarboxylase inhibitor. 03:20 A Dopa decarboxylase inhibitor will block L-dopa. 03:24 Dopa decarboxylase will prevent L-DOPA from being turned into dopamine and thus norepinephrine and epinephrine and subdue some of the effects that we see in the peripheral nervous system. 03:38 These days, it’s very common that L-DOPA and something like carbidopa are prescribed together for patients experiencing Parkinson’s disease, so a couple treatments that you should be aware of. 04:09 Now, another treatment that has got some pretty cool history behind it is with deep brain stimulation. 04:16 Initially, well, that’s just basically still what happens. We’d open up the brain. These super surgeries are actually fascinating to watch. They will enter the brain with an electrode and drop it into the substantia nigra and stimulate the neurons in the substantia nigra so that they secrete dopamine again. We’re reactivating, reenergizing neurons of the substantia nigra. 04:46 When this was first done, it was these pretty amazing surgeries because you would have someone with an open brain and electrodes going into the brain and people controlling mood. 05:00 It was kind of wild. Anyway, now it’s a little bit more common to see these deep brain stimulation technologies so much so that we now attach them to a pulse generator that can be implanted in the chest. Much like a pacemaker works on the heart, this pacemaker works in the brain with a constant pulse causing the neurons of the substantia nigra to secrete dopamine. 05:29 So, this in a lot of cases has been quite helpful. Although it’s not completely effective, it does have some good possibilities and potentials. Now, after this sort of research was done, they came around and started looking at stem cell therapies. That was sort of put on the back burner for political reasons and fetal stem cell and all of that stuff. But now that we have inducible pluripotent stem cell technologies, these research studies are becoming more invigorated and making their way towards clinical studies. Basically, in this case, we could take stem cells and plant them into the substantia nigra. Pretty successfully, they will regenerate dopaminergic neurons to replace those that have been destroyed. Really, really exciting possibilities in the realm of stem cell applications in treatment of Parkinson’s disease. So keep your eyes on that as you move forward in your practice.
About the Lecture
The lecture Parkinsonism and Treatment of Parkinson's Disease by Georgina Cornwall, PhD is from the course Aging.
Included Quiz Questions
How does co-administering a dopa decarboxylase inhibitor (DDCI, Carbidopa) with Levodopa enhance the treatment of Parkinson's disease?
- It blocks the peripheral conversion of Levodopa to dopamine, norepinephrine, and epinephrine, thus decreasing the adverse side effects of Levodopa.
- It acts as a direct dopamine agonist, at the cost of increased side effects of Levodopa.
- It is required for the transport of Levodopa across the blood-brain barrier.
- It acts as a direct dopamine antagonist peripherally, thus decreasing adverse side effects of Levodopa.
- It is a catalyst for the conversion of levodopa to dopamine once it crosses the blood-brain barrier.
Which statement is true about Deep Brain Stimulation (DBS) and dopaminergic/dopa-decarboxylase inhibitor (Levodopa/Carbidopa) therapies?
- Neither DBS nor dopaminergic/dopa-decarboxylase inhibitor therapies are definitive, but both provided limited symptomatic relief of the disease.
- Both DBS and dopaminergic/dopa-decarboxylase inhibitor therapies are definitive treatments for the disease.
- DBS is a definitive treatment for Parkinson's disease, while dopaminergic/dopa-decarboxylase inhibitor medication is simply for symptomatic relief.
- Both DBS and dopaminergic/dopa-decarboxylase inhibitor therapies stimulate the release of dopamine from neurons in the substantia nigra.
- DBS has far more peripheral side effects than dopaminergic/dopa-decarboxylase inhibitor medical therapy.
Which of the following is a type of primary parkinsonism?
- Parkinson's disease
- Brain injury
- MTPT contaminant in heroin
- Wilson's disease
- Progressive supranuclear palsy
Author of lecture Parkinsonism and Treatment of Parkinson's Disease

Georgina Cornwall, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
