Playlist
Show Playlist
Hide Playlist
Parainfluenza Viruses – Paramyxoviruses

-
02-45 Paramyxoviruses.pdf
-
Download Lecture Overview
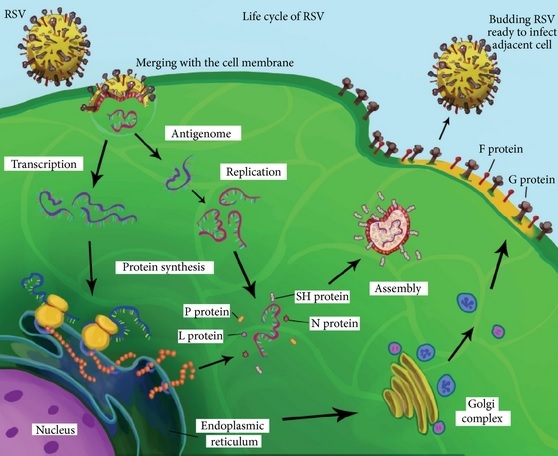
00:01 The parainfluenza viruses. Now we're going to the respiratory component of the paramyxoviruses. 00:07 These, of course, transmitted still by respiratory droplets and direct contact with those droplets. 00:13 Treatment is supportive for those patients who have respiratory distress. 00:18 One can use nebulized therapy, especially with those patients who have croup. 00:24 Providing warm, humidified air is a way to ease the turbulence of the air flowing through, and make it easier for the patients to breath. 00:32 Rarely, the patients require intubation and ventilation to get through the acute part of the disease. 00:39 There are 4 serotypes that we look at with parainfluenza. 00:43 Types 1 and 2, classically, are associated with croup, that seal bark cough that anybody who has children is quite familiar with. 00:52 Typically, kids from age 2-5 are the ones who are affected and infected by the parainfluenzas. 00:59 If the cough, which is due to laryngeal edema, tracheal swelling, if the cough progresses, then the patients may have inspiratory stridor, and that is when they come to medical attention and require the humidified air. 01:12 The chest X-ray may show a steeple sign on the frontal images, the PA or AP images. 01:19 And the steeple sign, although we don't have a picture of it in this talk, looks very much like the middle of my fingers. 01:26 So, right there, if you can see where my thumb is, is what the trachea looks like on plain film looking straight at that. 01:33 And that, of course, means that that patient is in danger of respiratory failure. 01:38 Serotype 3 for the parainfluenza cause croup, but more commonly, it causes lower respiratory disease. So bronchiolitis, pneumonia, and the pneumonia is going to be bilateral multilobar. 01:52 Typically seen in the extremes of age: the very young, the very old And then serotype 4, which is relatively uncommon, mostly causes a mild, upper respiratory tract infection, very much from - it's a cold. 02:06 So, then, respiratory syncytial virus. This is a biggie for anybody who practices pediatrics. 02:12 Transmitted via large respiratory droplets with direct contact. 02:16 In fact, patients with this disease when they're breathing out the droplets, typically spread them on many horizontal surfaces, which is unfortunate because we, as healthcare providers, come into the room, put our hands right on the horizontal surfaces, and then we typically scratch your nose or something, and then we have probably infected ourselves with respiratory syncytial virus, RSV. 02:40 Reinfection can occur. 02:42 There are different serotypes, and so one could get RSV infection twice in the season. The season is the winter season. 02:51 When reinfection occurs, thankfully, it is milder in symptoms, but adults still suffer from a bronchiolitis or lower respiratory tract infection with RSV, and they have a pronounced persistent cough. 03:03 Treatment is supportive. 03:07 There has been lots of evidence both for and against the use of bronchodilators, the use of aerosolized 3% saline. 03:15 But when all is said and done, the current approach is simply provide what the patient needs: oxygen, if they need oxygen, albuterol if they're wheezing, something like that. 03:26 For premature infants or patients with chronic lung disease, and especially infants in that stage, they benefit from the use of palivizumab. 03:37 It's a monoclonal antibody, specifically against RSV. 03:42 RespiGam was a prior product, which was a polyclonal approach, but the palivizumab is the way to go. And that has been quite protective against severe disease. 03:55 It doesn't prevent those infants from getting RSV, but at least if they do get RSV, they're less likely to have a severe progression of their disease. 04:04 What does RSV look like? In those of us who are adults, it's an upper respiratory tract infection with rare lower respiratory tract disease, unless we're reinfected. 04:15 And if it is upper respiratory, it is just like the common cold. 04:18 But the principal manifestation is in infants to toddlers with lower respiratory tract disease and they have bronchiolitis. 04:26 It is self-limited, thankfully. However, it is an overwhelming inflammation of the small airways, the bronchioles, which, as you can imagine, limits oxygen and gas transport, which creates respiratory distress, decreased ventilation. 04:42 And in any patient who has an immunocompromised state or preexisting lung disease, this can be an overwhelming process. And these patients will wind up on aggressive ventilatory support, or many times, ECMO, extracorporeal membrane oxygenation. 04:58 So, they're very sick and they look like it. 05:01 They'll have fevers, tachycardia, wheezes, or very limited air exchange, or air entry in their lungs, air trapping, the whole 9 yards. 05:10 So, RSV is a big deal in, especially young infants. 05:14 Recently, an RSV vaccine was approved for adults 60 years and older (with shared decision-making) and may be considered for patients within that age group who are at high risk for severe disease. 05:28 So I've given you a rundown of the paramyxoviruses. 05:32 Many viruses, many different effects depending on the tropism, where the viral infection goes. 05:38 If it's systemic, one gets incredibly systemic symptoms and signs. 05:42 If it's respiratory, one gets very aggressive respiratory disease. 05:46 So, this is a really good session to come back to, especially if one ends up going into a pediatric world for your career discernment.
About the Lecture
The lecture Parainfluenza Viruses – Paramyxoviruses by Sean Elliott, MD is from the course Viruses.
Included Quiz Questions
Which of the following is the treatment of choice for the management of infection by parainfluenza viruses?
- Supportive management
- Inhaled zanamivir
- Oral oseltamivir
- Inhaled ribavirin
- Oral baloxavir
Which of the following serotypes of parainfluenza viruses is most likely to be the culprit if an infant presents with bronchiolitis?
- 3
- 1
- 2
- 4
- 5
Which of the following do you expect to find on the chest X-ray radiograph of a child presenting with "seal bark" cough and inspiratory stridor secondary to infection by the parainfluenza virus?
- Steeple sign
- Bulging fissure sign
- Comet tail sign
- Finger-in-glove sign
- Westermark sign
Author of lecture Parainfluenza Viruses – Paramyxoviruses

Sean Elliott, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
