Playlist
Show Playlist
Hide Playlist
Neuromuscular Disease

-
Slides 03 NeuromuscularDisease Neuropathology II.pdf
-
Download Lecture Overview
00:02 Here, we’ll take a look at neuromuscular diseases. 00:04 Let’s begin. 00:06 But first, I want you to get an orientation of neuromuscular diseases, but before we do that, taking a section out of a spinal cord, I want you to move from your left. 00:17 We see a spinal cord. 00:19 And we’re going to amplify, amplify, amplify, from left to right. 00:23 I want you to orient yourself to the actual spinal cord where the anterior is on top. 00:29 Is that clear? But you knew that already because the anterior horn represents motor neuron, doesn’t it? And so therefore, we’ll talk about motor neuron diseases. 00:41 Not yet. 00:42 Because our topic here is neuromuscular disease. 00:46 Now as you move out from the motor, and you get into the CNS – or into the PNS, excuse me. 00:52 Then, we’ll start to talk about peripheral neuropathies and that’s the other big bracket that you see there. 00:57 But that’s not the topic yet. 01:00 I want you to move out from the peripheral nerve and then finally make it out to the muscle. 01:04 Ah! And then at that muscle is your neuromuscular junction. 01:10 And at that neuromuscular junction, we’ll talk about a few of these issue of neuromuscular diseases. 01:16 And at some point in time, when the time is right, we’ll talk about muscle itself undergoing disease and those are myopathies. 01:23 It’s a beautiful picture to give you an outline as to topics to come. 01:27 Motor neuron diseases and peripheral neuropathies, myopathies or even neuromuscular disease, which is our specific topic in this section. 01:38 Under neuromuscular disease, you can do degenerative as being a category. 01:42 And this is your Lou Gehrig or, a.k.a., amyotrophic lateral sclerosis. 01:49 With amyotrophic lateral sclerosis, let me give you a brief little introduction. 01:53 You’ll have motor issues only. 01:57 Sensory will be intact. 01:59 ALS. 02:00 Hereditary: a common one, known as spinal muscular atrophy or SMA. 02:06 And there’s one called Kennedy’s. 02:08 Under infectious, poliomyelitis and West Nile syndrome. 02:15 Let’s begin now our discussion by looking at amyotrophic lateral sclerosis or known as Lou Gehrig’s disease. 02:21 What happens? You only lose your motor, but of what type? Loss of upper and lower motor neuron in anterior horn of the spinal cord and in the corticospinal tract. 02:33 So what happens? You result in muscle atrophy and hyperreflexia. 02:38 Remember, you’ll have both lower and upper motor neuron type of lesions. 02:42 Amyotrophic lateral sclerosis. 02:44 What about sensory? Intact. 02:46 If you want, go back to that picture, that schematic that I showed you where we move out from the anterior horn and then come out through the motor, and then hit the neuromuscular junction. 02:58 With Lou Gehrig’s disease, the majority are sporadic and idiopathic. 03:02 There is a familial type that you want to memorize here, a genetic locus at your superoxide dismutase 1 or SOD1 gene on chromosome 21, which is a copper-zinc superoxide dismutase. 03:16 And this may account for 5 to 10% of your genetic cases. 03:19 Know that it exists and please make sure that you memorize a familial form. 03:23 But most, most, are idiopathic, unfortunately. 03:28 Clinical features: Remember, motor, motor, motor. 03:31 It’s asymmetrical weakness of hands. 03:34 So nonsymmetrical, early. 03:36 That’s important. 03:36 Pay attention to early manifestation. 03:39 Decreased muscle strength and bulk. 03:41 Remember both upper and lower motor neuron type of lesions. 03:45 Fasciculations, what does that mean to you? Involuntary contraction of individual motor units. 03:51 Progressive muscle or muscular atrophy to the point where the patient may not even have the ability to properly contract their diaphragm. 04:00 Not good. 04:01 And respiratory arrest. 04:03 Look for a patient who also has decreased ability to have a gag reflex. 04:09 Decreased muscle bulk especially noticeable in the thenar eminence. 04:14 That’s an important clinical feature. 04:17 Clinical features both mixed upper and lower motor neuron lesions that we talked about. 04:22 Some patients have degeneration of lower brain stem type of cranial nerve issue. 04:27 And may have progressive bulbar palsy or bulbar “ALS.” On electrophysiology, what are we going to find? Remember now, you’re going to see as to what the muscle activity is going to be like. 04:43 There are several disease-modifying treatments used in the management of ALS. 04:47 Riluzole has several potential mechanisms of action and has been shown to slow functional decline and improve survival by about 2–4 months. 04:54 Edaravone is a free radical scavenger which reduces oxidative stress, and sodium phenylbutyrate-taurursodiol is a histone deacetylase inhibitor which can reduce neuronal cell death. 05:05 Both of these may also slow the rate of functional decline. 05:09 There is not solid cure here, just keep this one in mind. 05:12 It is FDA-approved. 05:14 Symptomatic and supportive treatments are essentially what you’re going to do. 05:19 The course itself can be highly variable from individual to individual. 05:23 That’s extremely true. 05:26 You can have some patients that have ALS and you might not even know it because they’re actually functioning at a normal level. 05:34 Average lifespan, however, upon diagnosis is 5 years. 05:39 So that’s extremely grim. 05:42 Summary: Risk factors: Male preponderance, genetic. 05:47 Preventive: Really nothing that we know of truly. 05:50 Signs and symptoms: Weakness, atrophy, fasciculations. 05:54 Motor, motor, motor dysfunction only. 05:56 Upper and lower. 05:57 Remember fasciculations, individual muscle fiber type of twitching. 06:02 I shouldn’t use the word twitching, but contractions. 06:05 Mixed upper and lower motor neuron type of issues. 06:08 Diagnostic workup, you’re going to use electrophysiology to absolute seek decreased conduction. 06:14 MRI of the brain and spine, serology, lumbar puncture just to make sure that you rule other things out. 06:20 Management: Disease-modifying medications, And we have supportive care being essentially what you’re going to do. 06:29 We’ll come back to this picture again and this time, once again, as we go through this section, you’ll get a better idea as to how to orient yourself to the different classifications of neuromuscular diseases. 06:41 The first that we did was amyotrophic lateral sclerosis and there was a problem with the motor neuron, wasn’t it? And you had both upper and lower motor neuron lesions. 06:51 Next topic is going to be peripheral neuropathy, let’s take a look. 06:56 The pattern classification, we call this radiculopathy, involvement of the spinal nerve root. 07:03 Be familiar with the definition. 07:05 Radiculopathy characteristically is painful. 07:10 At some point, we’ll get into our -- well, you’ve heard of brachial plexus, obviously, or lumbar plexus. 07:17 So here, we’ll talk about what’s known as plexopathy. 07:20 It’s a pretty interesting name, isn’t it? Either the brachial or lumbosacral. 07:25 Mononeuropathy, involvement of a single nerve as the name implies, mono-. 07:32 And then you have mononeuropathy multiplex, what does that mean? It’s very important. 07:36 Involvement of one nerve but in multiple, multiple, locations or systems. 07:42 Mononeuropathy multiplex versus mononeuropathy. 07:48 Let me give you an example. 07:49 You have a medium to small vessel disease known as polyarteritis nodosa. 07:53 Polyarteritis nodosa. 07:56 And oftentimes, you’ll find the complex, the mononeuropathy multiplex. 08:04 We’ll talk about that in greater detail. 08:07 Polyneuropathy: As the name implies, multiple, symmetric involvement of peripheral nerves. 08:13 Our topic, peripheral neuropathy. 08:17 Usually in a length dependent fashion. 08:20 We call this stocking-glove type of distribution. 08:25 The pathologic classification for peripheral neuropathy. 08:28 Axonal. 08:29 Characterized by degeneration of axon. 08:31 Demyelinating characterized by loss of myelin. 08:34 Small fiber symptoms where there’s neuropathic pain, loss of pain and temperature sensation or maybe even autonomic dysfunction, peripheral neuropathy. 08:43 Or large fiber symptoms and this then includes weakness, diminished reflexes, loss of vibration, joint position. 08:51 So we have small fiber versus large fiber. 08:54 And here, once again, neuroanatomy will come in very handy here. 08:58 Two different types of classifications.
About the Lecture
The lecture Neuromuscular Disease by Carlo Raj, MD is from the course Other Diseases: Hydrocephalus, Neuromuscular Disease, Plexopathy, and Mononeuritis. It contains the following chapters:
- Neuromuscular Disease
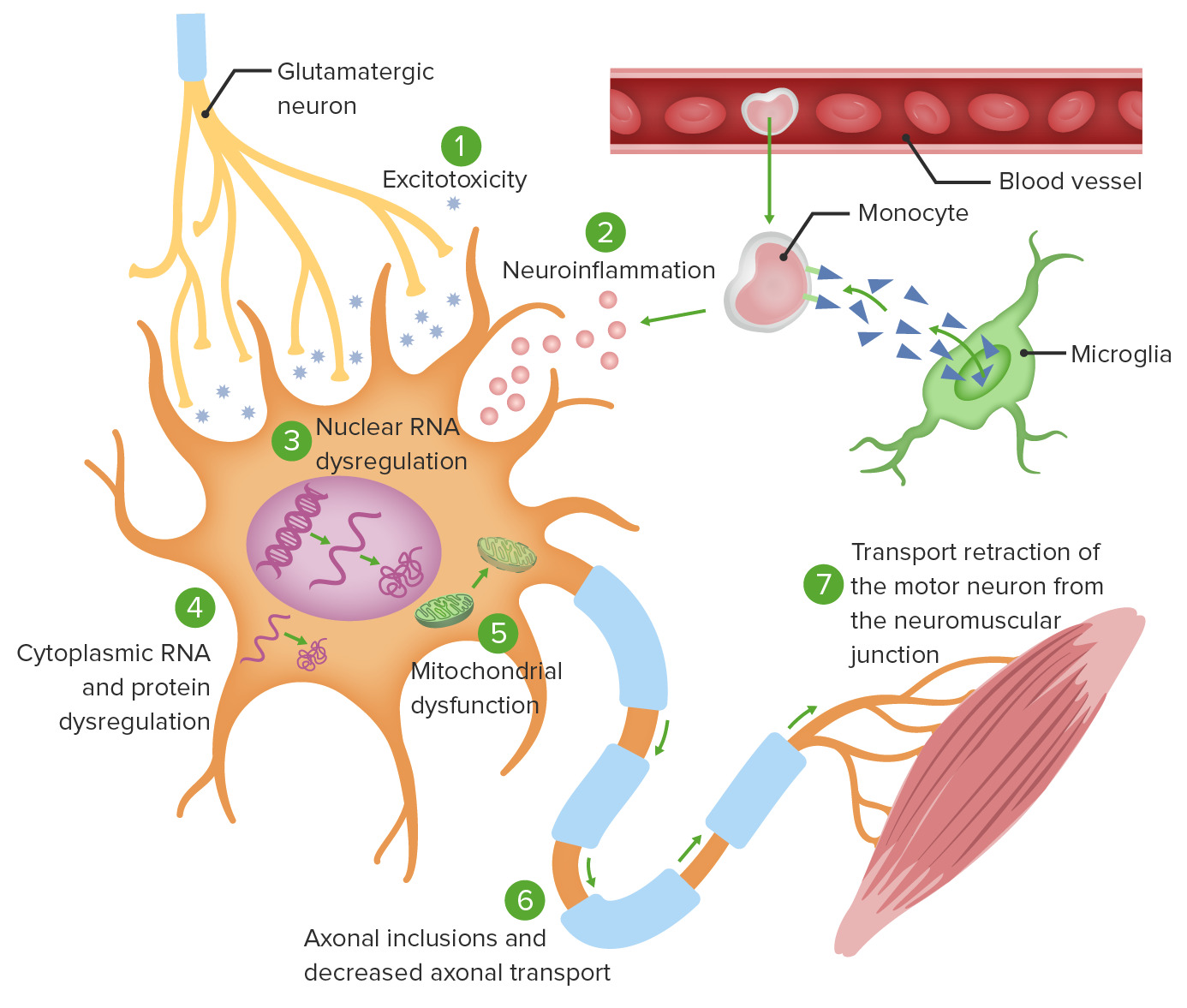
- Amyotrophic Lateral Sclerosis
- Peripheral Neuropathy
Included Quiz Questions
Which of the following findings is most characteristic of amyotrophic lateral sclerosis?
- Atrophy
- Loss of only upper motor neurons
- Loss of only lower motor neurons
- Hypertrophy
- Hyporeflexia
Mutations in which of the following genes are linked to the development of familial amyotrophic lateral sclerosis?
- SOD 1 gene on chromosome 21
- SOD 1 gene on chromosome 13
- SOD 1 gene on chromosome 22
- SOD 2 gene on chromosome 21
- SOD 2 gene on chromosome 9
Which of the following medications can improve the survival rate in patients with amyotrophic lateral sclerosis?
- Riluzole
- Methotrexate
- Infliximab
- Anakinra
- Amitriptyline
Which of the following is the most common presentation of amyotrophic lateral sclerosis?
- Asymmetric limb weakness
- Difficulty in breathing
- Fasciculation
- Dysphagia
- Dysarthria
Author of lecture Neuromuscular Disease

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
