Playlist
Show Playlist
Hide Playlist
Mitochondrial, Inflammatory, Endocrine and Drug Induced Myopathies

-
Slides 07 PolyneuropathyIndusIntellect Neuropathology.pdf
-
Download Lecture Overview
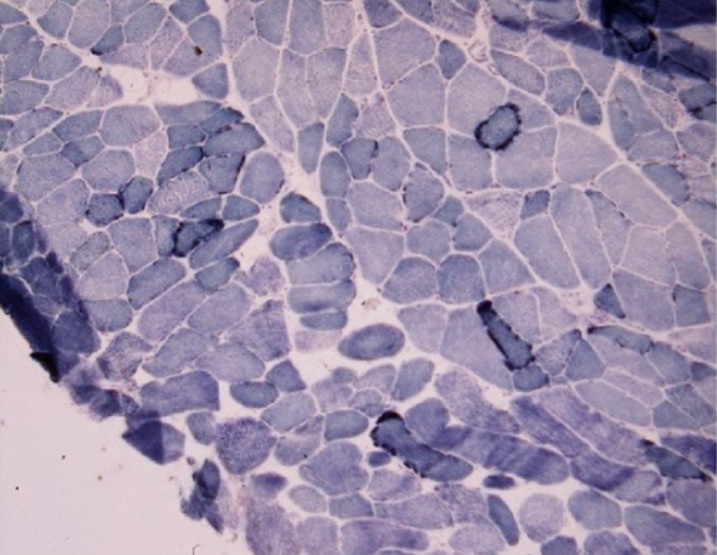
00:01 We’ll walk through a few mitochondrial myopathies. 00:03 To begin with, remember, in us, as you carry out as humans, we have two different types of DNA, right? We have our somatic or our nuclear DNA and then we have our mitochondrial DNA. 00:16 Our mitochondrial DNA is something that we inherit from mama, right, from our mothers. 00:20 So here, we have a couple of one’s that we have to know about, definitely know about. 00:24 Mitochondrial encephalopathy with lactic acidosis and stroke like symptoms, in other words that’s MELAS. 00:31 The other one is - pay attention to RRF. That’s ragged red fiber. 00:37 These are the ones that you’ve also talked about in biochemistry hence I am not elaborating on the abbreviation. 00:44 Either maternal inherited or sporadic, mother can be unaffected carrier though. 00:51 Frequently accompanied by other neurologic manifestation for example MELAS, mitochondrial encephalopathy, lactic acidosis and what S stands for? Stroke-like symptoms. 01:03 Muscle biopsy may show ragged-red fibers called RRF which represents peripheral collections of mitochondria. 01:12 Our topic here is inflammatory myopathy. 01:17 Begin by looking at dermatomyositis. Allow the name to speak to you. What do derm mean? Skin. 01:22 What do myo mean? Muscle. Hence we are doing our skeletal-muscle diseases. Then we have polymyositis. 01:31 And finally we have our, what known as our inclusion body myositis, in other words, inflammation. 01:37 Shoulder and hip girdle weakness is present, oh! Be careful! There is actually a condition that we called what? Limb and hip girdle myopathies or excuse me, dystrophies. 01:51 So be careful with those, right, versus here we’re dealing with shoulder and hip but after giving you further detail as well your clinical picture, don’t worry. 02:02 Relative sparring of once again the ocular and bulbar, and cardiac myopathy once again less frequent. So those are non-specific. 02:10 We see these earlier with limb and girdle muscular type of dystrophy. 02:14 So what is it about this conditions that is more specific? Let’s take a look. 02:20 First, we’ll take a look at dermatomyositis. 02:23 What are you gonna find? Well, when seen in adult often associated with underlying malignancy. 02:29 Derm, we’ll begin with the skin. Around the eyes, you have something called the heliotrope rash. 02:35 So its purplish discoloration of the eyelids, memorize that, dermatomyositis. 02:42 The first manifestation is going to be skin, more common in children, if it’s adult then it’s malignancy. 02:48 And then we have what's known as Gottron lesion and this Gottron lesion are going to be that around the knuckle. 02:55 It’s erythematous which means what? Red, scaly lesion over the knuckles, in other words your metacarpophalangeal joints. 03:02 Associated cardiac conduction abnormality, congestive heart failure or perhaps even interstitial lung disease. 03:09 Just keep those in mind because not only could you have then your skin issues, you can have issues with muscles as well. 03:16 Dermatomyositis, it is steroid responsive. 03:20 Here we have polymyositis. These are more common in older individuals. 03:28 Condition, steroid responsive. All that I wish to say about polymyositis. 03:34 Inclusion body myositis. Late-middle age to elderly predominance. 03:38 I just wanna make sure that you've heard of such conditions. 03:41 Early weakness of finger flexors and ankle dorsiflexors. Steroid resistant, inclusion body myositis. 03:51 Here we’ll take a look at endocrine myopathies. 03:55 The patient may have thyrotoxic myopathy often subclinical, brisk reflexes in other words it could be increase in thyroid hormone and you have creatine kinase typically would be normal versus hypothyroidic type of myopathy. 04:12 So think about decrease T3, T4. Proximal weakness, fatigue, myalgia, delayed relaxation; think of your patient with hypothyroidism everything slow down. 04:22 Creatine kinase is moderately to severely elevated. 04:25 Steroid myopathy could be caused by either endogenous or exogenous causes. CK is typically normal. 04:33 With drug and toxin induced myopathy, there are too many causes to list, but here are some important ones. 04:40 HMG CoA reductase inhibitor, your statins, do not forget may then cause necrotizing what’s known as rhabdomyolysis. 04:48 You'd find your creatine kinase to be ridiculously high obviously not very common but something very much to keep in mind. 04:55 Fluorinated glucocorticoids or dexamethasone. Alternate day dosing lessens the risk. 05:00 Remember that by taking steroids at every possibility that a myopathy could set in. 05:05 Zidovudine. Your patient is on highly active antiretroviral therapy, heart regimen. 05:14 There’s a possibility with mitochondrial myopathy with Zidovudine, AZT. 05:19 Cimetidine. H2blocker maybe patient is suffering from a gastric ulcer and so therefore you wanna block the acid production and in the process may result in inflammatory myopathy, keep that in mind, along with obviously gynecomastia and such.
About the Lecture
The lecture Mitochondrial, Inflammatory, Endocrine and Drug Induced Myopathies by Carlo Raj, MD is from the course Polyneuropathy. It contains the following chapters:
- Mitochondrial Myopathies
- Inflammatory Myopathies
- Endocrine Myopathies
- Drug/Toxic Induced Myopathies
Included Quiz Questions
What of the following statements about mitochondrial myopathies is true?
- They are maternally inherited or sporadic.
- They are paternally inherited.
- The mother cannot be a carrier.
- The father is a carrier.
- Ragged red fibers are composed of microtubules.
What do the ragged red fibers represent in MELAS?
- Peripheral collection of mitochondria
- Central collection of mitochondria
- Peripheral collection of microtubules
- Central collection of microtubules
- Peripheral collection of maternal DNA
A 10-year-old boy presents to your office with weakness for the past several days. On examination, a purplish hue is noted around the eyelids along with red papules on his knuckles. Which of the following is the most likely diagnosis?
- Dermatomyositis
- Limb-girdle muscular dystrophy
- Duchenne muscular dystrophy
- Becker muscular dystrophy
- Inclusion body myositis
Which of the following myopathies has normal levels of creatine kinase?
- Thyrotoxic myopathy
- Hypothyroid myopathy
- Duchenne muscular dystrophy
- Limb-girdle muscular dystrophy
- Myotonic dystrophy
A 55-year-old man is diagnosed with hyperlipidemia. In addition to lifestyle modification, he is started on a course of statins. Which of the following side effects should be monitored?
- Necrotizing myopathy
- Mitochondrial myopathy
- Inclusion body myositis
- Inflammatory myopathy
- Endocrine myopathy
Author of lecture Mitochondrial, Inflammatory, Endocrine and Drug Induced Myopathies

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
