Playlist
Show Playlist
Hide Playlist
Bivalirudin & Warfarin (Coumadin)

-
Slides Hematology-Pharmacology.pdf
-
Download Lecture Overview
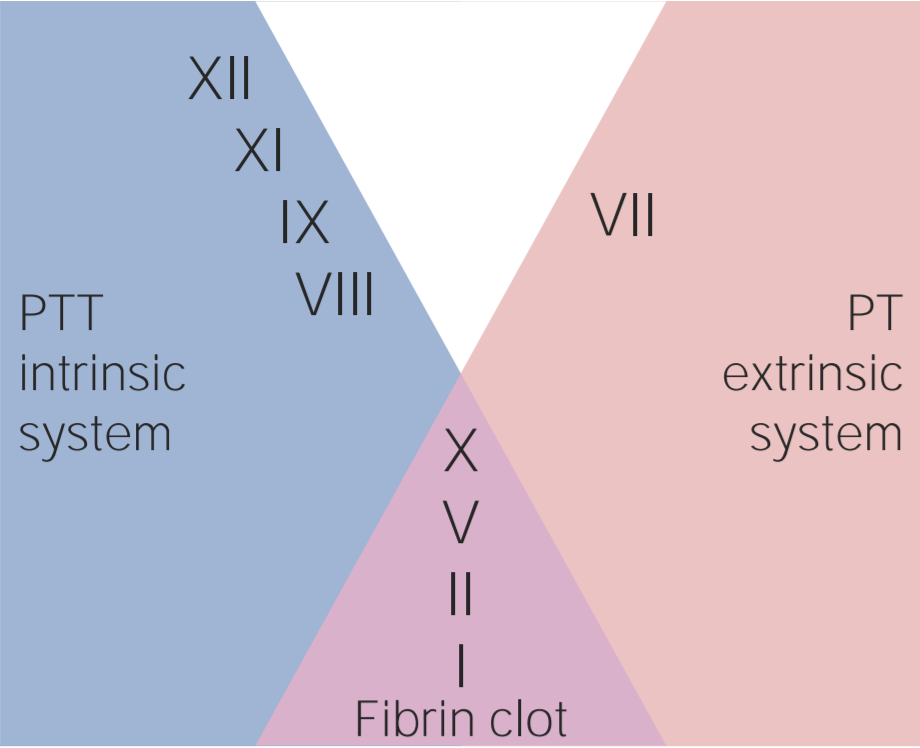
00:01 Here, we’ll take a look at two mechanisms of anticoagulation -- two. 00:08 The first one would be once again a direct acting thrombin inhibitor or thrombin inhibitors, and the other one would be the warfarin or a.k.a. Coumadin. 00:18 We have any suffix that you find with -udin, u-d-i-n, then you should be thinking direct acting thrombin inhibitor, I am being dramatic there because I want you to know that -uidin is going to be a direct acting thrombin inhibitor. 00:36 In addition, also, make sure that you know about an oral anticoagulant known as dabigatran; that would be the only one that is a direct acting thrombin inhibitor that you take orally. 00:49 There's another one called argatroban, but it’s dabigatran that could be given orally. 00:53 Now, the problem is this and you may be in a state of excessive anticoagulation and when that happens there is an antidote that you must know, it’s called idarucizumab. Idarucizumab, keep that in mind, please. 01:05 I also told you that with this direct acting thrombin inhibitors it could be an alternative to heparin if a patient was to then develop heparin induced thrombocytopenia, keep that in mind. 01:16 Let’s go and talk about that warfarin. 01:19 Now, why would you even considered giving warfarin? Well, let’s say that here once again we have a patient that is in a state of thrombi formation. 01:27 Maybe it’s a DVT and obviously we can't keep the patient on heparin forever, not a good thing and so therefore we need to release the patient from the hospital and when they go home they can now then take Coumadin, or warfarin orally. 01:41 That’s one situation right at home. 01:44 Or you have a patient who's elderly and has heart disease, maybe has some kind of angina, stable maybe even perhaps acute coronary syndrome. 01:53 Well, if that’s to take place then obviously here you wanna make sure that there's every possibility that you take a look at the ECG in such a patient, you find not only that the heart rate here might be a 150 beats per minute but you take a look at the -- you're trying to look for a sinus rhythm, in other words you're trying to look for that P-wave and it’s not there. 02:12 In other words it’s fibrillated and obviously I'm bringing to your attention atrial fibrillation. 02:17 Well, now, that you've created such a turbulent flow within your left atrium shall we say, there's every possibility that you've now developed a thrombi in the left atrium, think about that, please. 02:27 And if that thrombi ever embolizes where are you going? Well, we talked about this earlier but embolization most of the time would go down to the lower extremity, no doubt. 02:36 Approximately 75% of the time it would go to the maybe to the renal artery or to the super mesenteric artery. 02:42 Okay, well, that’s complicated, but what's devastating is that if it ever embolize up in the carotid, imagine if that happen, if embolize into the carotid then your patient now is developing a stroke or your cerebrovascular accident. 02:57 So therefore, warfarin has been proven over and over again effectively to be a prophylactic drug in a patient who has atrial fibrillation, specifically for preventing a stroke, cerebrovascular accident. 03:11 Now there are a couple of alternatives as well that I’ll give you in a second, but before that let’s talk about the mechanism how, here I need you to pay attention. 03:19 First, warfarin. 03:22 Warfarin works on your vitamin K dependent factors. 03:26 Vitamin K epoxide is the naturally occurring reduced or inactive form of vitamin K. 03:32 It is converted to its active reduced form, vitamin K hydroquinone, by vitamin K epoxide reductase or short VKOR. 03:42 Vitamin K hydroquinone is a necessary cofactor in the carboxylation of specific glutamate residues within the vitamin K-dependent proteins factors II, VII, IX, and X, and protein C and S – a process which is necessary to activate them. 04:02 The carboxylation reaction is catalyzed by gamma-glutamyl carboxylase. 04:08 Vitamin K hydroquinone is oxidized to the epoxide form during the carboxylation reaction, and recycled back to its hydroquinone form by VKOR. 04:18 Warfarin inhibits VKOR so vitamin K cannot be recycled from its oxidized form to its reduced form, and the vitamin K-dependent proteins therefore cannot be activated. 04:32 Now what could happen is the following: here molecularly, here’s some recent information that you wanna know. 04:37 You can have plasma polymorphism in that enzyme called vitamin K dependent epoxide reductase complex 1, in other words vitamin K, VKO, epoxide reductase complex 1-- that’s the actual molecular protein. 04:56 If your polymorphism in that enzyme, then maybe perhaps the warfarin may or may not be as effective in that particular patient, is that clear? Once you've understood that then, where does warfarin work? Or these Vitamin K dependent factors, how many times have we discussed this? My goodness, there's six of them total, correct? And I've told you over and over again to keep four of them separate from the other two - II, VII, IX, and X are prothrombotic and the C and S, you wanna keep separate cuz those are anticoagulants. 05:31 Let’s talk about that protein C and S. 05:33 Protein C and S are anticoagulants. It particularly works on immobilizing or in other words it cleaves your factor V, that is how that works. I want you to focus on factor V, I’ll tell you why in a little bit. 05:47 But protein C and S are anticoagulants and the half life of that or of them are very, very short. 05:54 You put all of these together and here’s my issue. 05:57 So, here’s warfarin. Take a look at the first sentence. 06:01 It says inhibition or disrupting normosynthesis. 06:04 What if in this particular patient the protein C and S is either deficient or the half life is so short it’s completely, completely depleted. 06:12 Oh, my goodness what do you have left in circulation, there you go, the prothrombotic agents right, which are II, VII, IX, and X and the theory is that you may then develop micro-emboli up and down the body. 06:26 If that’s the case then tell me where the necrosis would be? You have wide spread warfarin induced skin necrosis. That’s an issue. 06:33 There's a mnemonic that I gave you earlier called WEPT, W, warfarin. E, take a look at the e stands for extrinsic pathway, and PT is the test that you're gonna measure. 06:46 Now we've had this discussion as well in which two, I get it, thrombin is the convergent point, right? All, both intrinsic and extrinsic would through factor X activate prothrombin, no doubt, VII is part of the extrinsic, okay, that make sense, then IX really is part of intrinsic so why is it that PTT isn't elevated now? Please note, clinically, what’s significant and what you're only going to follow is going to be warfarin with PT/INR and that’s - the half life is much, much, much longer. 07:18 Not only that, but in terms of its toxicity, you are worried about the warfarin waging war upon the fetus so you wanna remove the warfarin in a pregnant lady obviously . 07:31 Now, the clinical uses we've talked about already with anticoagulation and so therefore we also said that it’s an oral agent, you follow the PT/INR. 07:40 You're thinking about the prophylaxis with a stroke in a patient that has atrial fibrillation and with warfarin though a couple of things here. 07:48 It’s the fact that it may then bring about skin necrosis. 07:51 So I told you that there might be alternatives, this is true. 07:54 So up until now we've talked about dabigatran a few times, the drug that is a thrombin inhibitor but what about one in which it may inhibit directly factor X? What's the letter -- what's in Roman numeral for factor X? X, X, and I told you earlier that for the most part, if you find an X in your drug such as apixaban or rivaroxaban or fondaparinux, then that would be a drug that inhibits factor X as a possible alternative to warfarin with dealing with prophylaxis of a stroke in a patient with atrial fibrillation.
About the Lecture
The lecture Bivalirudin & Warfarin (Coumadin) by Carlo Raj, MD is from the course Hemostasis: Basic Principles with Carlo Raj.
Included Quiz Questions
Which of the following anticoagulants is only available in the oral form?
- Dabigatran
- Hirudin
- Heparin
- Lepirudin
- Bilvalirudin
Which of the following best describes the mechanism of action of warfarin?
- Inhibition of synthesis of vitamin k dependent factors
- Inhibition of antithrombin 3
- Direct inhibition of thrombin
- Potentiating the neutralizing action of antithrombin 3
- Inhibiting cyclooxygenase
Which of the following proteolyses peptide bonds in activated factor V and regulates anticoagulation?
- Protein C
- Fibrinogen
- Prothrombin
- Tissue factor
- Factor XIII
Which of the following is a side effect of warfarin caused by acquired protein C deficiency?
- Skin necrosis
- Culture negative bacterial sepsis
- Intracranial hemorrhage
- Autoimmune hepatitis
- Alopecia
Which of the following is the most appropriate anticoagulant in a patient with atrial fibrillation due to a mechanical heart valve?
- Warfarin
- Dabigatran
- Enoxaparin
- Argatroban
- Fondaparinux
Author of lecture Bivalirudin & Warfarin (Coumadin)

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
