Playlist
Show Playlist
Hide Playlist
Lambert-Eaton Myasthenic Syndrome (LEMS) and Botulinum Toxin

-
Slides 07 PolyneuropathyIndusIntellect Neuropathology.pdf
-
Download Lecture Overview
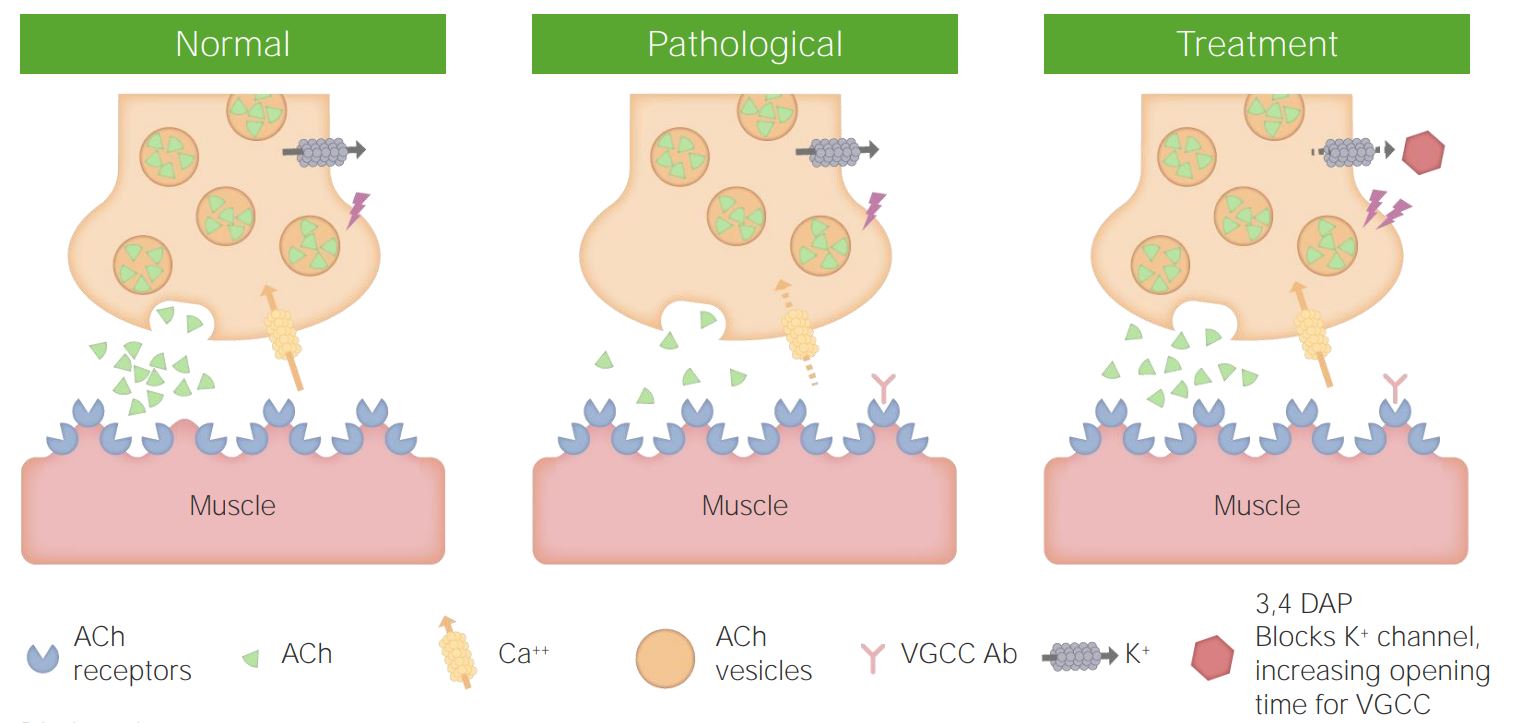
00:01 Lambert-Eaton myasthenic syndrome. 00:03 Before we begin, where are you? Once again, neuromuscular junction. 00:08 Now, once you’re dealing with the neuromuscular junction, then proximal muscles would be affected more so than the distal. 00:15 Now, this one is even more interesting. 00:18 The reason I say that is, well, these days are long with recordings, right? And these days are long in general in medicine. 00:26 But the way that I function is as the day progresses, I get stronger. 00:31 Why? Well, it’s not that I have Lambert-Eaton myasthenic syndrome, but that’s how that patient is going to be behave. 00:38 “Doc, I wake up in the morning and I feel like crap.” And then what happens? As the day progresses, I keep getting stronger and stronger and stronger. 00:47 So, where is my weakness and what’s my problem? The problem is presynaptically. 00:52 So now, I need you to think about what happens physiologically when you’re trying to release your acetylcholine. 00:58 You need action potential to then open up the voltage-gated calcium channels. 01:02 What’s voltage-gated calcium channels? Bring in the calcium and then you have fusion of your acetylcholine vesicles with the presynaptic terminal. 01:11 You then release acetylcholine and then you bind to your acetylcholine receptors. 01:15 As the day progresses, the body is going to find a way to release that acetylcholine. 01:20 Listen, your body is going to find a way to release that acetylcholine, which means what? You have no problem with the receptor, do you? Nope. 01:31 You don’t have a problem with the receptor. 01:33 So, acetylcholine will bind to the receptor, and once it does so, then you’re going to elicit an action potential. 01:38 Seventy five percent have an autonomic symptom, which are frequent. 01:42 For example, dry eyes, dry mouth, impotence. 01:46 Interesting. 01:47 Pupils can be involved, parasympathetic dysfunction, perhaps, because it’s a problem with the voltage-gated calcium channels. 01:54 That’s the issue. 01:55 And that voltage-gated calcium channel is not going to be as specific, right? As it was from myasthenia gravis where it was specifically the autoantibodies were attacking the acetylcholine receptors at the neuromuscular junction. 02:12 Deep tendon reflexes reduced or absent. 02:15 And muscle facilitation with brief exercise. 02:20 What’s interesting is the fact that if you’re able to promote movement, that there’s every possibility that the patient is actually going to get stronger. 02:28 Fascinating! And please don’t forget, it’s a part of paraneoplastic. 02:34 Pathophys: Let’s put everything together. 02:36 Autoantibodies directed against the presynaptic voltage-gated calcium channel. 02:45 Strong association with underlying malignancy. 02:49 I’ve mentioned this a few times. 02:51 Paraneoplastically, you definitely want to consider small cell lung cancer. 02:57 What does those small cell release paraneoplastically, potentially? ADH and ACTH, good. 03:05 Your nerve conduction test, decremental response with low frequency repetitive stimulation. 03:10 True. 03:11 The same thing that you would find with myasthenia gravis. 03:14 Here, incremental response with high frequency repetitive stimulation or after brief exercise. 03:21 That’s an important point. 03:23 You get stronger. 03:26 Management: Treat the underlying malignancy if it’s discovered. 03:31 Less successful than in myasthenia gravis, unfortunately: steroids, steroid-sparing agents, perhaps, and by that we mean immunomodulators, if necessary, IVIG, and plasmapheresis, if we’re getting into more of a crisis mode. 03:48 Our topic here very quickly is botulinum toxin, and we put things into perspective. 03:53 I live in Southwest, Florida. 03:54 Stereotypically, we have old people living there. 03:57 And for the most part, you walk around Fifth Avenue in Naples and you find your patients pretty much look like this. 04:04 All right, they’re walking around like this, and they have tons of wrinkles, but they really -- actually, they don’t. 04:09 They’re walking like this because they go into a clinic to get shot up by Botox. 04:15 In other words, you’re getting shot up by botulinum. 04:17 And what are you trying to do? These patients are trying to get rid of their wrinkles, aren’t they? And so therefore, I tell myself, “You look better with the wrinkles as opposed to looking like you have a masked face.” But whatever, to each their own. 04:33 Next, how do you get rid of the wrinkles? Well, you’re inhibiting the release of acetylcholine from the presynaptic terminal. 04:40 It’s what the botulinum toxin does. 04:42 But of course, your modification, you get this Botox. 04:46 But keep that in mind though, huh? What if you had a baby that was exposed to botulinum? What happens? Floppy baby, right? Floppy baby. 04:56 Why? Because the acetylcholine is not being released. 04:59 The incubation period is 18 to approximately 38 hours, so a couple of days, but can be as little as two hours. 05:06 Next, weakness is diffuse, as I told you, symmetric, proximal, once again, more so than distal. 05:15 Here, there could be issues with dilated pupil as well because why? It’s non-specific. 05:20 So, with botulinum, the toxin itself, it’s going to inhibit the release of acetylcholine everywhere, huh? Everywhere. 05:28 And the toxin interferes with presynaptic release of acetylcholine. 05:32 That’s your mechanism of action, either by the toxin or let’s say cosmetically, huh? Cosmetically.
About the Lecture
The lecture Lambert-Eaton Myasthenic Syndrome (LEMS) and Botulinum Toxin by Carlo Raj, MD is from the course Polyneuropathy. It contains the following chapters:
- Lambert-Eaton Myasthenic Syndrome (LEMS)
- Botulinum Toxin
Included Quiz Questions
A 45-year-old man presents to your clinic with fatigue and weakness. He does not have any medical conditions, but he complains that he feels extremely weak early in the morning and starts feeling energetic as the day progresses. What is the most likely site of pathology in his condition?
- Presynaptic voltage-gated calcium channels
- Postsynaptic voltage-gated calcium channels
- Presynaptic voltage-gated potassium channels
- Postsynaptic voltage-gated sodium channels
- Presynaptic voltage-gated sodium channels
Which of the following is NOT a feature of Lambert-Eaton myasthenic syndrome?
- Bulbar and ocular complaints are frequent.
- Bulbar and ocular complaints are rare.
- Autonomic symptoms are frequent.
- Deep tendon reflexes are reduced or absent.
- Muscles are facilitated with a brief exercise.
Which of the following is seen on nerve conduction studies in Lambert-Eaton myasthenic syndrome?
- Incremental response with high-frequency repetitive stimulation
- Incremental response with low-frequency repetitive stimulation
- Decremental response with high-frequency repetitive stimulation
- Decremental response after brief exercise
- No response with high-frequency stimulation
What is the most common malignancy that is associated with Lambert-Eaton myasthenic syndrome?
- Small-cell lung cancer
- Squamous cell carcinoma of the lung
- Large-cell lung cancer
- Pheochromocytoma
- Hodgkin lymphoma
Which of the following statements regarding botulinum toxin is true?
- It blocks the presynaptic release of acetylcholine.
- It blocks the postsynaptic release of acetylcholine.
- It is neither foodborne nor inhaled.
- It presents with asymmetric weakness.
- Miosis is common.
Author of lecture Lambert-Eaton Myasthenic Syndrome (LEMS) and Botulinum Toxin

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
