Playlist
Show Playlist
Hide Playlist
Hypothalamic Hormones


-
Slides CellTypesHormones EndocrinePathology.pdf
-
Download Lecture Overview
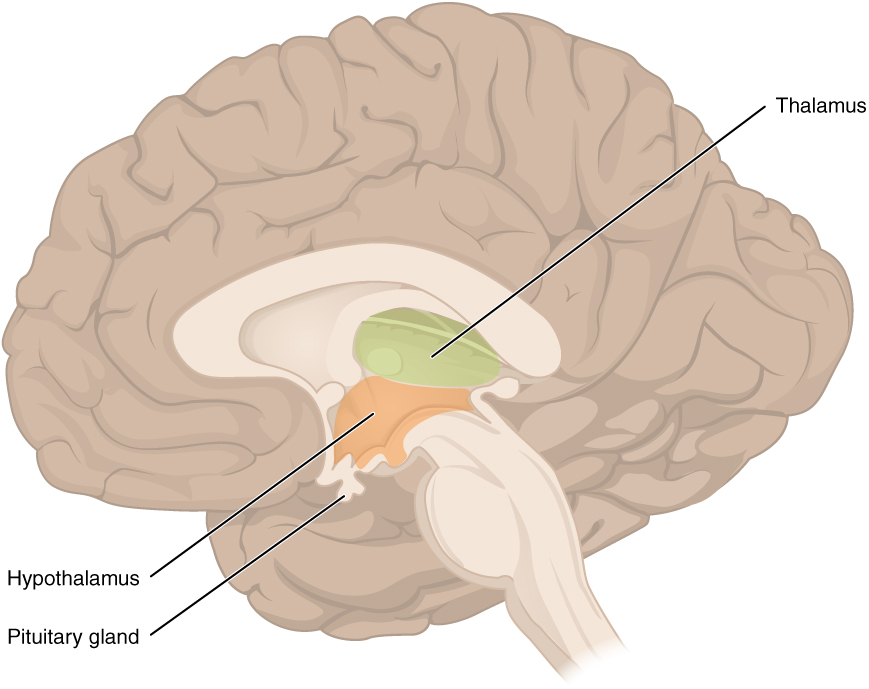
00:01 Next, what we’re going to do here is begin at the level of the hypothalamus and quickly, just reiterate those releasing hormones for you. 00:11 In the first portion of endocrinology, I then walked you through the group of releasing hormones and I gave you a picture. 00:21 But, what I’m going to add in here as well is some clinical applications and integrations. 00:25 So, let’s go and dive into this a little bit further, shall we? First, growth hormone releasing hormone. 00:34 It works upon the anterior pituitary to release what? I’m sorry I can’t hear you. 00:39 Growth hormone, good. 00:41 What inhibits growth hormone? Somatostatin, right? Somatostatin, why is that important? Analog of somatostatin could be used in what kind of patient? Acromegaly. 00:57 What else? Well, the medicine available include what’s known as your tesamorelin. 01:00 Keep that in mind. 01:02 This is a growth hormone releasing hormone analog… tesamorelin. 01:08 Somatostatin, I just gave you a couple of examples in which you inhibit or you wish to inhibit growth hormone release… acromegaly. 01:18 Welcome to your drug octreotide. 01:21 Do not confuse this with somatotrophs or somatomammotropins. 01:27 Corticotropin-Corticotropin releasing hormone. 01:30 Now, a couple of things here that you want to pay attention to. 01:34 Remember, your boards current day practice and current day boards is not about you memorizing, you’re only going to get so far with memorization. 01:44 Obviously, the 200 and 205 you’ll be desperate for residency program; 227 you’re competitive… you’re competitive; 240/250, you own, haha, this residency programs, right? They want you, you’re not begging. 02:06 So, what do you want to do on this exam? Think… critical thinking. 02:12 You can’t memorize this stuff. 02:15 Corticotropin releasing hormone, I can give you a lot of angles so that you can get your 240 and 250 and that’s why you’re here. 02:25 CRH promotes ACTH. 02:27 Okay, no big deal, but the next one’s interesting. 02:31 Cortico-Corticotropin releasing hormone stimulation test to distinguish, you fill in the gap, you fill in the gap between primary, secondary, adrenal insufficiency, right? Think. 02:48 If it’s primary adrenal insufficiency, I don’t… and-and you give… you give corticotropin releasing hormone, primary. 02:57 You’re going to release ACTH, but there’s no effect because the adrenals are dead, right? Addison’s. 03:06 Next, corticotropin releasing hormone in secondary adrenal insufficiency, where is my problem? Anterior pituitary, secondary. 03:15 You with me? What does primary mean? Primary from med school means that primary organ is never able to release that hormone. 03:25 Where should cortisol come from? Adrenal cortex, Addison’s is a primary. 03:30 So, no matter how much CRH did you give, ACTH will be released, but you’re not going to have cortisol. 03:38 In secondary, my problem is in the anterior pituitary, it gives corticotropin releasing hormone. 03:45 Now, at this point, your ACTH is not going to be released; it will be decreased. 03:51 In both cases of primary and secondary adrenal insufficiency, your cortisol levels will be depressed, but for different reasons, right? Because you know in primary, your ACTH levels are elevated whereas in secondary, even with a CRH stimulation test, you find your ACTH to be depressed. 04:11 If you’re still not good with that, that’s okay, I’m just introducing the concept that you need to make sure that you iron out properly. 04:20 And as we go into details of the adrenal cortex, I’ll point it out one more time or plus repeat, haha, and then listen to what I just said again. 04:28 Alright, let’s go on to TRH. 04:31 Where are these coming from, these hormones? Right, hypothalamus. 04:34 Where are they working? Good, in the anterior pituitary. 04:40 Target? All over the place, huh? And you need to be sport about that. 04:45 TRH works upon where? Once again anterior pituitary. 04:48 What are you going to release? TSH. 04:51 Stop, that’s the easy part. 04:53 Let’s say that you give TRH… not give TRH, your patient has elevated levels of TRH. 05:01 Why? Oh, Hashimoto… Think Hashimoto… primary hypothyroidism. 05:06 What’s your TRH-TRH levels? Whoop, increased. 05:10 What about prolactin? Whoop, increased. 05:12 Welcome to hyperprolactinemia, right? Do not forget that, TRH. 05:16 Not only does it release TSH, also releases prolactin, therefore it’s a female. 05:22 Tell me about her menstrual cycle, present or not present? Good, not present. 05:27 Clinically, we call this amenorrhea. 05:30 Next, theoretically, once again, another angle, huh, maybe a pathophysiology question. 05:36 Theoretical confirmation of secondary and perhaps tertiary. 05:40 What does that mean to you? What if you give TRH here and it’s secondary hypothyroidis? What do you mean secondary? If it’s secondary hypothyroidism, where is my problem? Once again, it will be the anterior pituitary, right? Where’s primary hypothyroidism? Thyroid. 05:58 Secondary hypothyroidism? It will be the problem in the anterior pituitary. 06:03 You give a TRH stimulation test and guess what? You are not able to properly stimulate my anterior pituitary to release TSH. 06:10 Clear? So, you want to walk through that. 06:13 Now, technically speaking, tertiary means the third place where you can have a problem with decreased T3/T4. 06:22 The first place, primary, thyroid; second place, anterior pituitary; third place, tertiary would be where? Hypothalamus. 06:31 Be able to think through all of endocrinology and really all of medicine and there’s no way that the boards can really fool you. 06:38 Maybe one or two questions here and there just because you got tired, you know, but apart from that though, you’ll be okay. 06:43 Let’s take a Gn... 06:45 Let’s take a look at GnRH, gonadotropin releasing hormone. 06:48 What’s interesting about a lot of these hormones, I will tell you, is the fact that they’re pulsatile. 06:55 A lot of these are pulsatile in nature, what does that mean? Remember I told you that a lot of your hormones are being released at night when you’re sleeping including growth hormone that’s why you use IGF1? Also GnRH pulsatile, what does that mean? [sound] It’s like a beat… boom, boom, boom, boom… just like a drum. 07:15 And every time you hit that drum is when you release that hormone, pulsatile in nature. 07:20 That’s important for you to know, isn’t it? Oh yeah, watch this. 07:25 Before we begin though, GnRH, releasing hormone, come from hypothalamus, working where? Anterior pituitary. 07:30 What it releasing? LH and FSH. 07:34 Depending as to what gender? If it’s a male, obviously the testes; if it’s a female, it will be the ovaries, right? Now, when it’s a short-acting analog is known as a gonadorelin, the brandname... look at this, it’s called Lutrepulse, why the pulse? Now you know. 07:55 Why the “L”? Lutre. 07:57 Well, you know because this wasn’t before releasing LH and such. 08:00 Gonadorelin is important. 08:02 You also have a long-acting analog. 08:04 This is the one that you definitely want to know. 08:06 This is leuprolide. 08:07 Now, what does this mean? Remember pulsatile, that is perfect, optimum rhythm. 08:12 Here you are in the rhythms of studying, right? All of a sudden there is a bulldozer coming through the… coming through your home [sound], right? Ha-ha! And so, now, at this point, it completely disrupts your rhythm and so, therefore, whatever studying that you’ve been doing is down the drain. 08:30 What I mean by that is literally, if you were to step your foot on the pedal, long-acting... 08:38 at first, you’re going to have increased stimulation, but please know that everything in the anterior pituitary is going to be destroyed or slowed down if you continue pressing on the pedal. 08:53 This is leuprolide. 08:54 In order for you to inhibit the release of LH and FSH from the anterior pituitary, you do not give an antagonist... or excuse me, you can give an agonist... yes, you can give an antagonist, but you give an agonist so that you lose the pulsatile rhythm of release and you have constitutive down regulation of your receptors. 09:17 Thus LH and FSH will be decreased, but initially, you’re going to have a stimulus, initially. 09:24 So, that stimulates and suppresses FSH and LH release respectively. 09:29 That statement should be very clear to you now and you’re not just memorizing it. 09:34 Stimulating, stop. 09:35 Yes, initially transient. 09:38 What’s your ultimate goal? Obviously to suppress. 09:42 Why is this important? Well, in management and pharmacology and such, you’ve talked about things such as prostate cancer and you’ve talked about management of polycystic ovarian syndrome and so, therefore, leuprolide is a drug to suppress release of LH and FSH. 09:59 Interesting, isn’t it? Then you have other drugs here. 10:02 A pure gonadotropin releasing hormone antagonist and this is your Degarilex.
About the Lecture
The lecture Hypothalamic Hormones by Carlo Raj, MD is from the course Pituitary Gland Disorders.
Included Quiz Questions
What is the function of octreotide?
- Inhibiting secretion of growth hormone
- Inhibiting secretion of somatostatin
- Increasing secretion of growth hormone releasing hormone
- Increasing insulin sensitivity
- Increasing insulin-like growth factor 1 levels
Which condition is most likely to have decreased adrenocorticotropic hormone (ACTH) and cortisol levels?
- Trauma to the anterior pituitary
- Addison disease
- Cushing disease
- Cushing syndrome
- Acromegaly
Which type(s) of hypothyroid state(s) present(s) with low thyroid-stimulating hormone and thyroid hormone levels?
- Secondary and tertiary
- Secondary
- Primary, secondary, and tertiary
- Primary
- Primary and secondary
Which drug suppresses the release of luteinizing and follicle-stimulating hormones when administered continuously, mainly by interrupting the pulsatile release pattern of gonadotropins?
- Leuprolide
- Gonadorelin
- Tesamorelin
- Degarelix
- Octreotide
Author of lecture Hypothalamic Hormones

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
