Playlist
Show Playlist
Hide Playlist
Heart Sounds – Cardiac Cycle


-
Slides CardiacCycle CardiacPhysiology.pdf
-
Download Lecture Overview
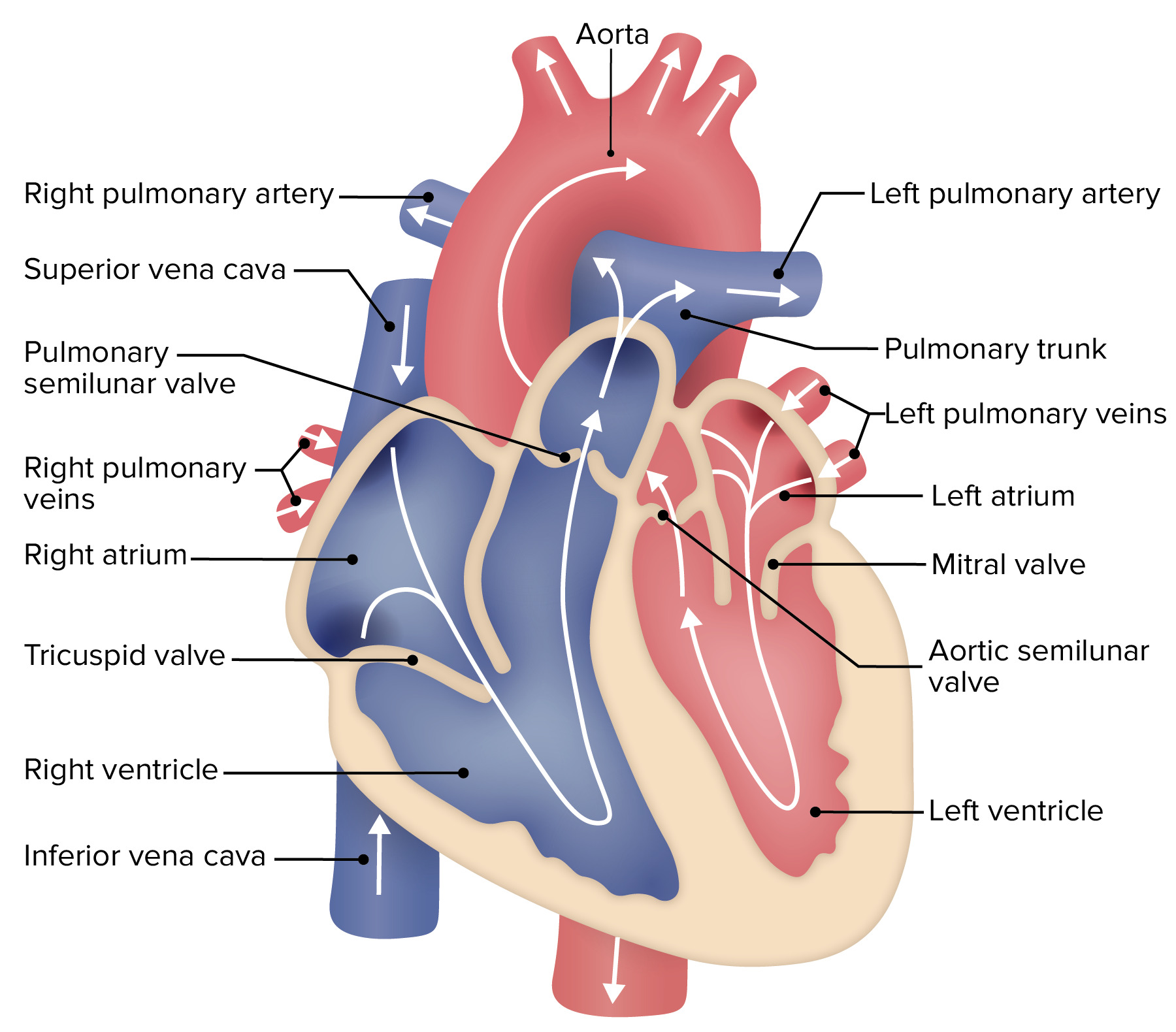
00:01 So far, we’ve really only talked about blood pressure and volume. 00:07 Now, we’re going to introduce another concept that’s really important for you clinically. 00:13 You know this inherently in the inherent lub-dub sound of the heart. 00:18 You can put a stethoscope on someone's chest and listen to heart sounds. 00:23 This is one of your clinical items that you can try to make sure that you’re understanding how the heart is functioning. 00:33 So, let's go through what are the heart sounds that you can hear. 00:36 The first one is known as S1. 00:40 This involves when the mitral, which is the bicuspid, and the tricuspid valves close. 00:47 They close about at the same time. 00:51 This is around the same time as the QRS complex and it's during isovolumic contraction. 00:59 There's a little bit of a split sound, in that the bicuspid valve, which is also known as the mitral, precedes the tricuspid valve closing just by a very short timeframe. 01:13 The next sound that you hear is when the aortic and the pulmonary valves close. 01:20 This occurs along the ECG just after the T wave and is about at the same time as isovolumic relaxation. 01:29 This gives you two insights. 01:31 You can think of isovolumic contraction and isovolumic relaxation as being times when you hear S1 and S2. 01:41 This happens when those valves close. 01:45 The aortic valve precedes the pulmonary valve closing by just a split second. 01:51 This allows for there to sometimes be a split sound in the stethoscope listening of those sounds. 01:59 So, you might hear two different S2 sounds. 02:04 Now, why are these sounds important? Well, if you think about having the mitral valve and tricuspid valves close, if a person has a murmur in these two valves, you can hear it around S1. 02:19 If there is a murmur around S2, you know, maybe the aortic or the pulmonary valves have a murmur. 02:26 A murmur can be quite serious. 02:28 Anything from a stenotic valve to a valve that is prolapsed or is leaking. 02:37 Other heart sounds that you can hear, one is called S3, which is known as early diastolic filling. 02:45 So, this occurs during the rapid filling phase of the left ventricle. 02:51 It is normal to have in children. 02:55 However, if you have a dilated left ventricle, it is pathological. 03:01 So, someone that has a dilated cardiomyopathy presents with an S3 sound. 03:07 So, for those individuals, you will listen and hear an S1, hear an S2, and then hear an S3 before you get back to the S1. 03:15 The last heart sound is known as an S4. 03:19 The S4 is associated with the atrial contraction. 03:23 This is caused by pushing blood into a stiff ventricle. 03:30 So, if the ventricle is not able to withstand or to fill when the top part of the heart is contracting, that creates the sound. 03:41 It especially occurs in people that have hypertrophy in their hearts, whether it be left ventricular hypertrophy or right ventricular hypertrophy, and it can also happen as individuals age because the ventricles become stiffer, just like blood vessels do. 03:58 At this point, I will mention one other thing about heart sounds because it's very easy to confuse. 04:04 Even though you're listening to the stethoscope through the person's chest, you might ask, well, what do you hear? You hear these sounds. 04:13 What does that refer to? You would like to think something like S1 and S2 are associated with actually hearing the valve close. 04:23 That's not what occurs. 04:25 The valves close and you hear the turbulence in the fluid associated with that valve closing. 04:33 You don't actually hear the leaflets hit. 04:36 So, that's a process that is good to think about that what you're listening for is turbulence in the fluid. 04:45 That makes S3 and S4 make more sense because if you have a lot of fluid going into a big ventricle, there’s more turbulence. 04:54 And as you hear more turbulence, it sounds like a sound. 04:58 If you're pushing something into a stiff ventricle, you create turbulence, and it’s that what you hear.
About the Lecture
The lecture Heart Sounds – Cardiac Cycle by Thad Wilson, PhD is from the course Cardiac Physiology.
Included Quiz Questions
Which heart sound is heard in early diastolic filling and may be an indicator of pathology?
- S3
- S1
- S2
- S4
- S5
Which of the following contributes to 2nd heart sound?
- Closure of aortic and the pulmonary valves
- The flow of blood from atria
- Contraction of atria
- Closure of AV valves
- Contraction of ventricles
Which of the following contributes to 1st heart sound during systole?
- Closure of AV valves
- Closure of semilunar valves
- Contraction of ventricles
- The flow of blood from atria
- Contraction of atria
Author of lecture Heart Sounds – Cardiac Cycle

Thad Wilson, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
He gets straight to the point, I liked this lecture. I recommend it
