Playlist
Show Playlist
Hide Playlist
Esophagitis esp. GERD


-
Slides GD Esophagus.pdf
-
Download Lecture Overview
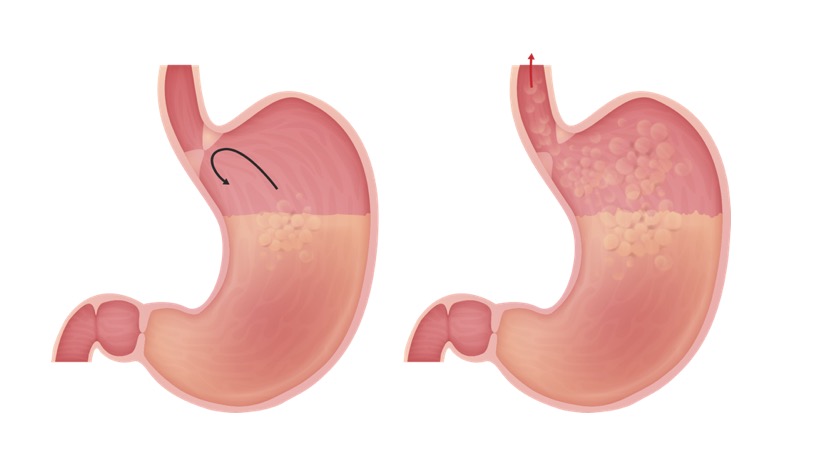
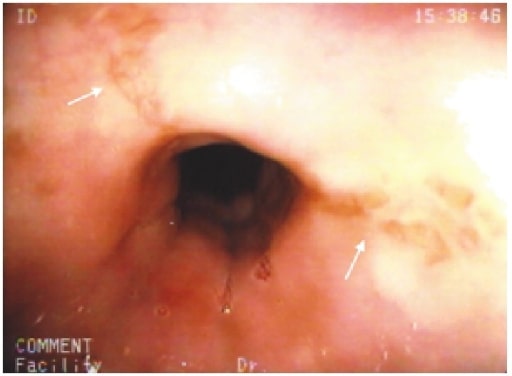
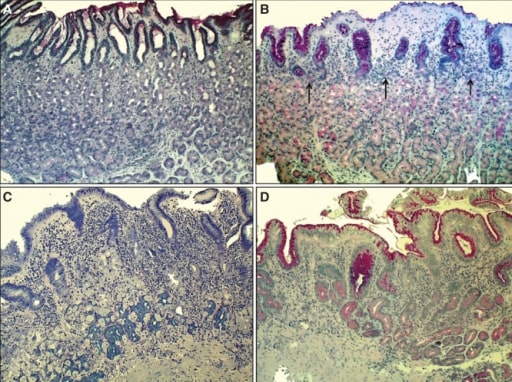
00:01 Let’s move on to esophagitis. 00:03 In general, a nice little overview of the different things we’ll take a look at with esophagitis. 00:08 GERD - we’ll take a look at symptoms, diagnosis, treatment. 00:11 Pill induced - for example if it’s NSAIDs and such, and aspirin over a long period of time you decrease the lining of the esophagus. 00:18 Caustic ingestion - And by that we mean that the patient is now taking up some type of chemical. 00:23 Infectious to you should mean immunocompromised. 00:28 Viral - maybe Herpes, Cytomegalovirus, HIV. 00:33 Immunocompromised. 00:35 Maybe bacterial, fungal, definitely, definitely immunocompromised. 00:39 You’ve heard of candidiasis, you’ve heard of oral thrush. 00:44 If you have a Candida infection of esophagus, you’ll have the same type of cottage cheese appearance. 00:50 Let’s begin. 00:52 Reflux esophagitis is what we are, GERD is my topic. 00:57 Reflux disease. 00:59 Gastroesophageal Reflux Disease, we had talked about this and discussed as to how a patient as an adult may then have hiatal hernia, at the level of T10. 01:08 This reflux over a long period of time, with this acid coming back into the esophagus, may then bring about a metaplastic change. 01:17 Mean to say that the squamous cells of the esophagus may then turn into or undergo metaplasia into columnar cells. 01:27 If it continues from… this is then referred to as Barrett’s esophagus. 01:31 If this continues, and the patient is either non-compliant, and we’ll talk more about this later in steps of management. 01:38 For example, lifestyle modification is huge. 01:41 Don’t eat late at night. 01:42 When you go to sleep, angle yourself so that you do not… you prevent the reflux from taking place. 01:49 And try not to smoke, and so on and so forth. 01:53 But if the reflux continues to Barrett’s esophagus, which is not a cancer, but its metaplasia, is at risk for dysplasia and adenocarcinoma. 02:02 Common. 02:03 Associated with hiatal hernia as we talked about. 02:06 Or what if a patient has diabetes mellitus, and there’s something called gastroparesis and you don’t have proper emptying of your stomach? And then you might then result in reflux. 02:18 Transient relaxation of the lower esophageal sphincter, that’s my problem. 02:22 Excessive relaxation of the LES. 02:25 GERD has a more frequent transient relaxation and longer periods of that reflux. 02:31 See relaxation is a good thing. 02:33 It’s called your receptive relaxation. 02:36 Remember, there’s a test that you’ve seen in physio which is called manometry. 02:41 If you were to put a bolus into the mouth and get into esophagus, the pressure within esophagus rises. 02:50 As soon as you have a rise, physiologically, of pressure in the esophagus, this then triggers automatically relaxation of the lower esophageal sphincter because obviously peristalsis. 03:03 You want to get the food into the stomach. 03:06 However in GERD, there’s excessive relaxation. 03:09 Underlying cause remains unknown, potentially maybe perhaps one of you will end up finding it and go on to great praise. 03:20 The symptoms of GERD: If there’s reflux taking place, heartburn, “chest pain”, often times could be… well in your head as a differential you should be thinking about things such as myocardial infarction. 03:37 Dyspepsia, water-brash and dysphagia. 03:41 Dysphagia here reflux, difficult because of that chest pain. 03:45 And also, with all this acid reflux, there might be with enough reflux in the esophagus, may actually irritate the respiratory system. 03:53 And so therefore, your patient may complain of breathing issues, similar to that of asthma. 03:59 “Doc, for whatever reason, I feel like I’ve just developed asthma. 04:04 I’m having a hard time breathing at times." “Hmm." Along with this you go on to do a barium swallow and you end up finding issues with reflux. 04:16 Chronic cough. 04:18 Atypical symptoms. 04:20 The diagnostic evaluation of GERD: dysphagia; Testing not necessary for typical symptoms. 04:27 Weight loss, anemia, refractory symptoms, prolonged symptoms, atypical symptoms are extremely alarming. 04:35 So testing not necessarily for typical symptoms but recommended for “alarm” features. 04:41 The reason for this is because you’re worried about your patient going on to developing cancer of the esophagus. 04:48 What kind would this be most likely with GERD? You go from Barrett’s esophagus to metaplasia, into dysplasia and into your adenocarcinoma, most likely located in your lower esophagus. 05:05 May present as progressive dysphagia. 05:10 You start losing blood and such, you’re worried about iron deficiency. 05:13 The diagnostic evaluation’s important for you. 05:18 Quite a bit of a problem is GERD in the US, but because of proper diagnostic evaluation and screening methods, and hopefully the patient is compliant. 05:28 The incidence of adenocarcinoma in the US, thank goodness is dropping. 05:35 You’ll want to do a 24 to 48 hour pH monitoring; now we do this wirelessly. 05:41 Presence of esophageal damage, this you’re going to check out on endoscopic examination. 05:47 And the damage that you’re looking for here, we call Barrett’s tongue. 05:51 The Barrett’s tongues represents the metaplastic changes taking place of your squamous into columnar cells. 05:59 Symptoms correlation with reflux; for example, with something called the Bernstein test - the perfusion of esophagus with acid to induce the symptoms of GERD. 06:11 Such as, your coughing we talked about, the burning sensation in the chest, so on and so forth. 06:19 The complications of reflux: The barium swallow. 06:21 Well, what does damage that’s taking place with the esophagus due to the reflux, remember there’s strictures, means what to you? Increased repair process of the esophagus upon injury. 06:38 Of course reflux is injury. 06:40 So things that you’re looking for with the GERD as very common associated diagnoses include stricture formation. 06:51 And also I’d mention that hiatal hernia is also accompanying, accompanying issue with in fact reflux.
About the Lecture
The lecture Esophagitis esp. GERD by Carlo Raj, MD is from the course Esophageal Disease: Basic Principles with Carlo Raj. It contains the following chapters:
- Esophagitis
- Reflux Esophagitis
- Symptoms of GERD
- Diagnostic Evaluation of GERD
Included Quiz Questions
Which of the following is related to the histopathology of GERD?
- Relaxation or weakening of the lower esophageal sphincter (LES)
- Constriction of the lower esophageal sphincter (LES)
- Diffuse relaxation of the esophagus
- Diffuse constriction of the esophagus
- Weakening of the upper esophageal sphincter (UES)
Which of the following is MOST likely associated with GERD?
- Hiatal hernia and delayed gastric emptying (possibly from diabetes mellitus)
- Peptic ulcer disease
- Infection
- All of the above
What is the MOST common cancer that is predisposed by GERD?
- Metaplasia leading to adenocarcinoma
- Squamous cell carcinoma
- Lymphoma
- Sarcoma
- All of the above
What is the diagnostic test of choice used to evaluate the presence of reflux in a patient with GERD?
- 24–48 hour pH monitoring
- Endoscopy
- Barium swallow
- Surgical exploration
- None of the above
Which associated condition is a patient who presents with esophagitis due to viral or fungal infectious etiology MOST likely to have?
- Immunocompromised status
- Immunocompetent status
- GERD
- Pill-induced inflammation of the esophagus
- Alkali or caustic injury to the esophagus
Author of lecture Esophagitis esp. GERD

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
1 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
my favourite lecturer. great lecture on such a complex topic
