Playlist
Show Playlist
Hide Playlist
Common Fibular Nerve – Nerve Lesions of the Lower Limb

-
Slides 10 LowerLimbAnatomy Pickering.pdf
-
Download Lecture Overview
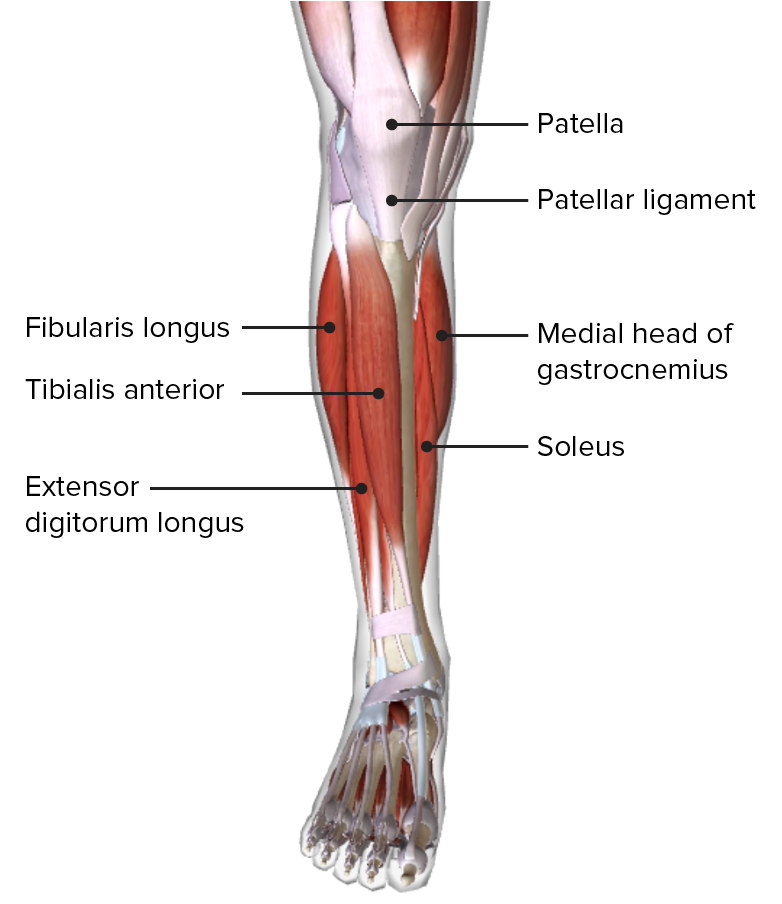
00:00 Now let’s turn to the common fibular nerve, and we know the common fibular nerve bifurcates from the sciatic. It then runs along the lateral border of the popliteal fossa, and it divides into the superficial and deep fibular nerves - the superficial nerve supplying the lateral compartment, the deep fibular supplying the anterior compartment. 00:23 So here, we can see that the neck of the fibula has the common fibular nerve wrapping around it. Now we know from a previous lecture that the neck of the fibula and the head of the fibula are very superficial and can easily be palpated. So this means that the common fibular nerve is prone to injury, as it’s located superficially around the neck of the fibula on the lateral aspect of the leg. Damage to the common fibular nerve is going to lead to flaccid paralysis of muscles in the anterior, the dorsiflexors, and the lateral elevators of the leg in the leg compartments, the anterior and lateral leg compartments. Those are responsible for dorsiflexion and eversion. With no dorsiflexion, you’re unable to lift your foot up. So you’re unable to lift your toes up keeping your heel on the floor, and therefore, you have foot drop. The foot drop assumes this permanent plantarflex position. So when you go to walk, you’re likely that your toes in this plantarflex position will drag along the floor as the limb becomes too long and it’s difficult for your toes to clear the ground. To compensate for this, you have this waddling gait where the body moves to the unaffected side, therefore, giving you clearance. You have a swing-out gait where the leg is excessively abducted to avoid the toe sitting in the floor. And you have this stepping gait where you have increased thigh and knee flexion to raise the foot higher up so it can then clear the ground.
About the Lecture
The lecture Common Fibular Nerve – Nerve Lesions of the Lower Limb by James Pickering, PhD is from the course Lower Limb Anatomy [Archive].
Included Quiz Questions
What are the 2 branches of the common fibular nerve?
- Superficial and deep
- Anterior and posterior
- Medial and lateral
- Major and minor
- Superior and inferior
Author of lecture Common Fibular Nerve – Nerve Lesions of the Lower Limb

James Pickering, PhD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
5 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
