Playlist
Show Playlist
Hide Playlist
Cerebral Aneurysm: Introduction


-
Slides 03 CerebralAneurysms Neuropathology I.pdf
-
Download Lecture Overview
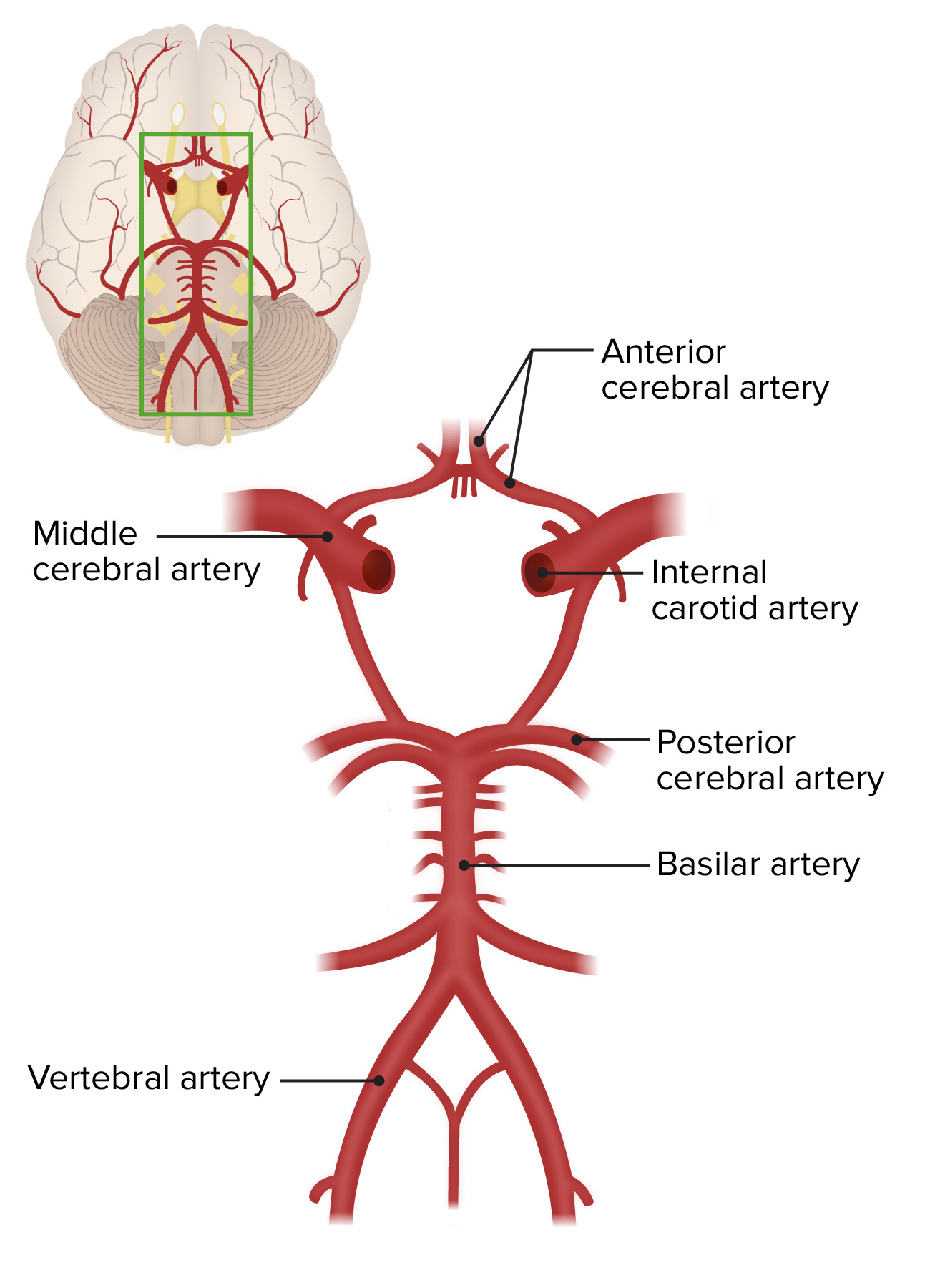
00:01 Hello and welcome to cerebral aneurysms. 00:05 In order for us to fully comprehend cerebral aneurysms, it’s important that you understand the anatomy of your circle of Willis. 00:13 And when, here, we refer to aneurysms, we’ll be strictly looking at the circle of Willis and so therefore the caliber of your blood vessels will be a little larger. 00:26 You’ll see what I’m referring to. 00:27 Let’s begin. 00:28 So here’s the circle of Willis and I'm not going to through the details obviously. 00:33 However, a few things that I wish to bring to your attention. 00:36 I want you to pay special attention to anterior communicating artery and the reason for that is because if there are aneurysms – What does an aneurysm mean to you? It’s a ballooning or expansion of your blood vessel, correct? And if there’s an aneurysm, at any point in time, you’re always worried about an increase in tension and pressure, resulting in a possible tear. 00:58 And that’s where we’re headed eventually, aren’t we? The reason that I bring anterior communicating artery to your attention is because, let’s say, 40 to 60% of your aneurysms will be taking place in the anterior portion of the circle of Willis. 01:14 And you should very well know that. 01:17 Apart from that, we have the large middle cerebral artery. 01:20 We have spent time with that earlier when we talked about strokes. 01:24 And then I want you to focus upon the basilar artery. 01:27 And from the basilar artery down below, we have the posterior inferior cerebellar artery. 01:32 All of these of course incredibly important when we’re dealing with strokes. 01:36 Each one of these will give you different symptoms in your patient. 01:40 With the berry aneurysm is what we look at here. 01:42 It’s also called a saccular aneurysm. 01:44 And by saccular, we mean that the entire wall, meaning to say the caliber, the circular nature of the blood vessel, every part of it has undergone weakening and so therefore, there’s a saccular aneurysm, a.k.a. berry aneurysm. 02:00 Rupture is the most frequent complication. 02:03 And so imagine anything that’s causing increased tension or pressure of your blood vessel or perhaps even weakening of the wall of the blood vessel such as Marfan or Ehlers-Danlos, could result in berry aneurysm and then eventually could rupture. 02:17 And when it does, of course, it is then causing hemorrhage into the subarachnoid space. 02:22 On a scale of one to ten, with ten being the worse possible pain that the patient experienced, the patient is definitely going to scale it as being ten. 02:30 Thunderclap. 02:31 We’ll talk about this as a separate topic in a little bit. 02:35 Whenever there’s hemorrhage that’s taking place, keep in mind of its proximity to the parenchyma of the brain, so therefore it could result in also intraparenchymal bleeding. 02:45 And that of course makes perfect anatomical sequential sense. 02:49 And as far as the rupture is concerned, most commonly, it would be found in the fifth decade You have probably already looked at and memorized autosomal dominant polycystic kidney disease with that increase in hypertension, and eventually resulting in berry aneurysm and rupture. 03:03 But apart from that, please make sure that you know anything that’s causing increase pressure even hypertension over a long period of time or weakening of the integrity of the blood vessel wall, will result in such an aneurysm and rupture as being a complication. 03:18 Larger aneurysms can present as mass lesion. 03:22 And symptoms will then result in compression type of neurologic structure issues. 03:28 It may result is such compression and therefore affecting the third cranial nerve and this of course referring to your oculomotor. 03:37 And when we say involving the pupil, please don’t forget from neuroanatomy, that when you’re dealing with cranial nerves, that you should also know as a mixed function, that there could be autonomic nervous system, specifically, the parasympathetic nervous system, correct? With the oculomotor. 03:54 And the if oculomotor has been lost, you have now also lost the ability to properly constrict. 04:01 And so therefore, you could have a blown pupil. 04:04 In other words, a mydriatic type of pupil. 04:07 If the pupil is spared, then like infarction of the nerve, seen in diabetes. 04:11 And that’s important, once again. 04:14 If the pupil has been spared, then likely infarction of the nerve secondary to diabetes. 04:22 Are we clear about this? A very important clinical point. 04:26 If the pupillary constriction has been lost centrally, then maybe there is a compression type of issue. 04:34 In this case, the large berry aneurysm is the cause. 04:39 But if the pupillary constriction is intact, that means that it’s more of a peripheral issue. 04:46 Infarction should come to mind. 04:49 For example, the infarction, therefore resulting in compromise of nerve activity, as in diabetes. 04:56 If you’re not familiar with that in neuroanatomy, please make sure that you’re very keen upon that point so that you can understand your clinical presentation. 05:05 It is a big deal. 05:07 Continuing our discussion of berry aneurysm. 05:09 The natural history of it. 05:10 If it was to rupture, it may result in SAH, stands for subarachnoid hemorrhage. 05:17 Now, once subarachnoid hemorrhage does occur, 2% of population maybe seen as being autopsy series. 05:23 Now, one thing that you’re definitely worried about is that this bleeding doesn’t stop. 05:28 Unfortunately, there could be a recurrent hemorrhage and remains a serious consequence and to a point where the case fatality rate is now nearing 70% for persons who are rebleeding. 05:40 That is a big deal. 05:41 Make sure that you digest that particular point, please. 05:44 Our topic, an aneurysm that has ruptured resulting in subarachnoid hemorrhage. 05:50 Now, in the prospective Cooperative Aneurysm Study, CAS, rebleeding was maximum, 4% on the first day after SAH and then constant at a rate of 1 to 2% per day over the subsequent 1 month. 06:07 And what does that rebleed mean to you? It increased the rate of mortality up to 70%. 06:12 You understand the significance? Long-term risk, 3% per year after three months. 06:18 So the risk does decrease if you’re able to properly manage them. 06:22 Please make sure that you’re quite aggressive in terms of how quickly this occurs or when you can expect the rebleeding, which is usually about first day, and then constant over the next following four weeks.
About the Lecture
The lecture Cerebral Aneurysm: Introduction by Carlo Raj, MD is from the course Cerebral Aneurysm (Intracranial Aneurysm).
Included Quiz Questions
What is the most common site for the development of a cerebral aneurysm?
- In the circle of Willis at the anterior communicating artery
- In the middle cerebral artery (MCA)
- In the posterior inferior cerebellar artery (PICA)
- In the basilar artery
- In the posterior cerebral artery (PCA)
Which of the following is an example of an anatomical abnormality in which the entire wall of the blood vessel undergoes weakening?
- Saccular or berry aneurysm
- Serpentine aneurysm
- Fusiform aneurysm
- Cylindrical aneurysm
- Racemose aneurysm
What is a potential complication of polycystic kidney disease?
- Subarachnoid hemorrhage (SAH)
- Epidural hematoma (EDH)
- Global ischemic stroke
- Lobar hemorrhage
- Focal ischemic stroke
Author of lecture Cerebral Aneurysm: Introduction

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
2 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
It was really Informative, well explained, enthusiastic, just great!!! Keep up the good work
The presenter is knowledgeable about the subject and presents the topic in an easy to understand and interesting manner!
