Playlist
Show Playlist
Hide Playlist
Acromegaly (Growth Hormone Excess)


-
Slides AnteriorPituirary EndocrinePathology.pdf
-
Download Lecture Overview
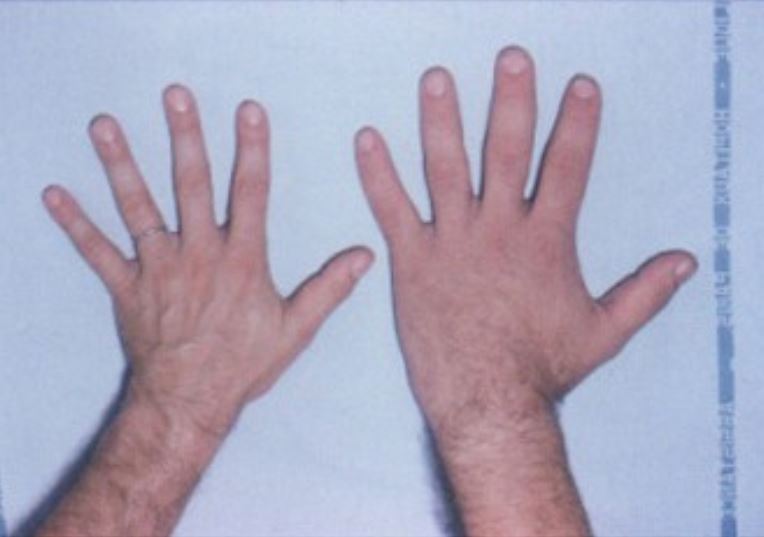
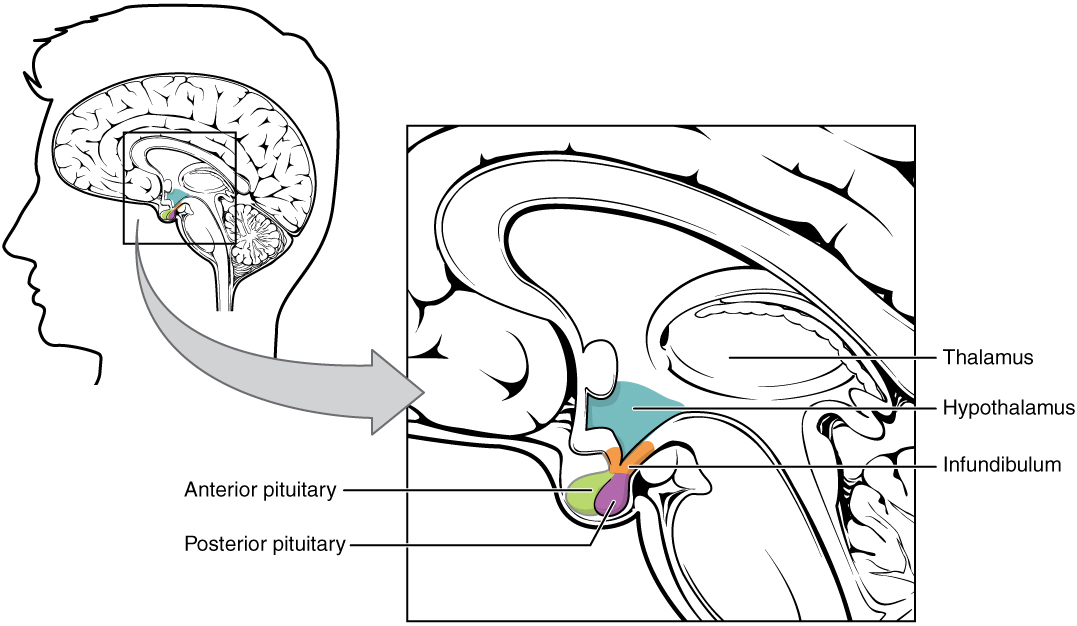
00:01 With growth hormone excess and acromegaly, take a look at your patient up above and to the right and we have frontal bossing. 00:08 If you take a look at the frontal area, you’ll find that the bone is protruding forward and you can actually notice prognathism in this patient as well. 00:17 Look at the jaw, extremely well demarcated. 00:20 You take a look at the patient down below and you find exaggerated prognathism in the patient that has acromegaly. 00:28 Excessive sweating; with all these growth hormone in an adult, you can then expect there to be hyperglycemia; there might be Carpal tunnel syndrome because of excess, as we’ve said, soft tissue issues… growth, growth, growth; high incidence of colon polyps co-relate with skin tags on exam and that’s something that you want to pay attention to from a clinical point of view. 00:51 Remember, acromegaly, you’re thinking about the internal organs that are growing including bones, the viscera, maybe the tongue, maybe the frontal bone, maybe the jaw and hyperglycemia. 01:03 Cardiovascularly, this is a patient that may then die from it. 01:08 Cardiovascularly, this is a patient that may then die from it. 01:09 Growth hormone from head to toe… enlarged head, enlarged sella, large and widely spaced teeth, protruding chin… prognathism; deep voice, blood pressure elevated, osteoarthritis, big feet… everything’s increased. 01:25 Whenever we suspect acromegaly in an adult, usually for you, it will be the presence of a adenoma within the anterior pituitary. 01:36 Invasion into the left cavernous sinus with encasement of the internal carotid artery is something that you would perhaps find in the MRI that we’re seeing here in this picture. 01:48 Superior bowing of the optic chiasm resulting in and I’ll show a cartoon down below which is then showing you bitemporal hemianopsia. 01:56 OD is the right eye, OS is the left eye and that, that you see as being squiggly lines on the temporal regions would be those areas in which the patient with a pituitary adenoma is not able to see those areas. 02:11 The pressure on the optic chiasm produces this particular picture or lack thereof. 02:19 Diagnosis of acromegaly... 02:20 I want you to focus upon the graph here and take a look at the X and Y axis. 02:25 On the X axis would be the time in minutes after oral glucose and what kind of effect and influence it should normally have on growth hormone which is the Y axis. 02:41 Before we dive into the pathology, let us first predict as to what you can expect normally so that when you take a look at the path, you’ll be able to easily identify your patient. 02:50 Okay, so, you have taken oral glucose, the usual dosage that we use in medicine is about 75 grams of bolus. 03:00 That’s a pretty big bolus orally of glucose that you’re taking. 03:06 What should happen normally in terms of being able to properly metabolize that glucose is to make sure that you inhibit as much as you can of the stress hormones and bring in your major anabolic insulin, right? So, what happens in acromegaly? Remember that growth hormone is a stress hormone. 03:30 So, therefore, after taking glucose, it should normally… take a look at the green line… over certain period of time, you find a drop in your growth hormone. 03:43 So, when you compare this to acromegaly, you’ll notice that after consumption of glucose that over period of time, huh, the growth hormone seems to have its own mind, autonomously increasing. 03:59 Diagnosis of acromegaly… screening. 04:02 Remember, it is not growth hormone that you are going to be looking for, it’s IGF1. 04:08 IGF-1 is generated by the liver in response to GH. 04:12 It is the mediator of the growth effects of GH. 04:17 For diagnosis acromegaly, IGF-1 is superior to GH because it has a longer half-life, without a pulsatile secretion like GH, so its levels are stable throughout the day. 04:28 Confirmation… non suppression of growth hormone after 30 minutes and 60 minutes of consuming OGTT, stands for Oral Glucose Tolerance Test. 04:46 We’ll be using this acronym a lot when we get into diabetes mellitus. 04:53 But, after administering glucose, you’ll notice the red line with growth hormone did not get suppressed… welcome to confirmation. 05:03 What’s your next step of management? Remember, previously I just, just told you that acromegaly usually represents an adenoma in the pituitary. 05:16 Thus, if you do an MRI of the head, you should be able to find a tumour. 05:21 What’s your goal? It’s to normalize your growth hormone IGF level. 05:27 Treatment of choice… treatment of choice transphenoidal surgery, cure 50 percent less likely with macroadenoma because of the size in the residual tissue that may actually exist. 05:42 Somatostatin analogue… octreotide… is adjunct to the medical treatment. 05:47 So, here, interesting enough, it is your transphenoidal surgery which would be the treatment of choice because of the size of the adenoma usually with growth hormone and that’s an issue. 05:58 Whereas if it’s a microadenoma, usually it would be prolactin that’s being released; macroadenoma more along the lines of your growth hormone and remember, the number one question that you ask yourself any time that there is an adenoma, “Is this functioning or non-functioning?” This obviously is functioning. 06:18 Acromegaly… what else? Also inhibits glucagon, insulin and gastrin; long acting synthetic analogue of somatostatin used to treat acromegaly, carcinoid, gastrinoma… this is a nice little list of octreotide and all the different indications in which you may want to use it. 06:39 Acromegaly, it inhibits serotonin and carcinoid; it inhibits gastrin and gastrinoma; it inhibits the glucagon and glucagonoma and other endocrine tumours. 06:54 So, from physio and endopathology and forevermore, think of somatostatin as being the hormone that inhibits all others from the head with GH and all the way down through your GI referring to carcinoid and also your gastrinoma. 07:15 The side effects… gall stone formation and some cardiac conduction abnormalities is something that you’re worried about as a result of acromegaly and treatment. 07:29 30 percent may response to cabergoline. 07:34 That was interesting. 07:36 Remember, whenever growth hormone is being released, there’s every possibility prolactin might as well and yes, some of these patients that will actually respond to dopamine. 07:48 We have a drug, a growth hormone receptor antagonist and it is called pegvisomant. 07:55 That’s a growth hormone receptor antagonist. 07:59 And what does it do? It inhibits and reduces IGF1 in 90 percent of your patients. 08:06 Radiation, only as adjunctive here, post-surgically once again to deal with perhaps the residual tissue.
About the Lecture
The lecture Acromegaly (Growth Hormone Excess) by Carlo Raj, MD is from the course Pituitary Gland Disorders.
Included Quiz Questions
What is NOT a common clinical manifestation of acromegaly?
- Sudden onset
- Sleep apnea
- Carpal tunnel syndrome
- Colon polyps
- Excessive sweating
What is the preferred initial screening test for diagnosing acromegaly?
- Measurement of serum IGF-1 levels
- Measurement of nocturnal GH levels
- Oral Glucose Tolerance Test (OGTT)
- Measurement of serum prolactin
- MRI of brain
What would NOT suggest the presence of a pituitary adenoma?
- Bilateral involvement of inner ear structures
- Invasive lesion of the left cavernous sinus
- Encasement of the internal carotid artery by lesion
- Superior bowing of the optic chiasm
- Bitemporal hemianopsia
What is a confirmatory test result for acromegaly?
- Non-suppressed GH levels 30 minutes and 60 minutes after glucose challenge
- Increased IGF immediately after glucose challenge
- A spike in GH levels after 30 minutes, which then declines before 60 minutes.
- Increased somatostatin in response to glucose
- Marked hypoglycemia due to GH increased after glucose challenge
Which drug is a growth hormone receptor antagonist?
- Pegvisomant
- Cabergoline
- Octreotide
- Somatostatin analog
- Radiation
Author of lecture Acromegaly (Growth Hormone Excess)

Carlo Raj, MD
Customer reviews
5,0 of 5 stars
| 5 Stars |
|
2 |
| 4 Stars |
|
0 |
| 3 Stars |
|
0 |
| 2 Stars |
|
0 |
| 1 Star |
|
0 |
Dr. Raj, you did a great job! Learned a lot!!! Thank you so much!
His lectures are related 100 percent to First Aid that's always helpful
